Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Psoriatic booklet 12 page.qxd
PSORIATIC BOOKLET 12 PAGE.qxd 2010/03/16 02:41 PM Page 1
What is in this booklet?
This booklet aims to answer questions commonly asked bypeople who have psoriatic arthritis. Each section deals with adifferent question. A brief answer (in italics) is followed by amore detailed explanation. What is psoriatic arthritis? Psoriatic arthritis causes inflammation in and around the joints,usually in people who already have the skin condition psoriasis. Sometimes, however, the arthritis develops before the psoriasis.
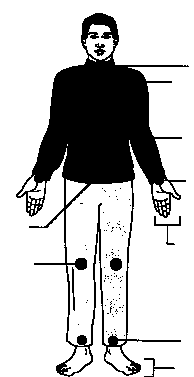
There are 78 major joints in the body and psoriatic arthritis canaffect any one of these. However, certain joints are more like-ly to be affected - these are shown in Figure 1. Different pat-terns are found. Sometimes it affects just one or two joints suchas a knee or ankle, but often several joints, both large andsmall and on both sides of the body, are involved. About athird of people with psoriatic arthritis also have a painful, stiffback or neck caused by inflammation in the spine. This iscalled spondylitis. Figure 1. Joints commonly affected by psoriatic arthritis
Psoriasis can affect the nails with pitting, discoloration andthickening. Sometimes the joint at the end of the finger or toecan also be inflamed. There can be a sausage-like swelling of afinger or toe with psoriatic arthritis.This is called dactylitisand is caused by inflammation occurring simultaneously injoints and tendons.Painful heels can be caused by inflamma-tion where gristle attaches to bone. Some of the symptoms of
PSORIATIC BOOKLET 12 PAGE.qxd 2010/03/16 02:41 PM Page 2
psoriatic arthritis are shown in Figure 2. Psoriatic arthritis usually affects adults but occasionally chil-dren can develop the disease. How does the doctor diagnose psoriatic arthritis? Psoriatic arthritis is diagnosed based on your symptoms and on whatyour doctor finds when s/he examines you. There is no specific testfor psoriatic arthritis.
Most doctors would check for psoriasis, or a history of psoria-sis in a close relative, together with arthritis and inflammationin at least one joint. It can be difficult to distinguish betweenpsoriatic arthritis and rheumatoid arthritis. If several jointsare affected doctors will consider features such as the patternof arthritis (which joints are affected) and other symptoms (see‘What is psoriatic arthritis?’) to distinguish between the twoconditions. Blood tests for rheumatoid factor, if negative, mayalso help to rule out rheumatoid arthritis. Can psoriatic arthritis attack other organs of the body? Usually, apart from the skin, nails and joints, no other major organsare affected.
People with psoriatic arthritis may be more likely to developan itchy, red eye due to conjunctivitis, and some people mayoccasionally develop a painful, red eye caused by inflamma-tion around the pupil of the eye. This is called iritis or uveitis. Some people may also develop anaemia (a shortage of redblood cells). Although this is not a specific feature of psoriat-ic arthritis it can sometimes happen as a result of long-terminflammation.
How common is psoriatic arthritis? Psoriatic arthritis is not common. About 1 in 50 people have psori-asis, and of these about 1 in 14 will develop psoriatic arthritis.
People with psoriasis may also have other forms of arthritis,such as osteoarthritis or rheumatoid arthritis, but these are notlinked to the psoriasis and are not dealt with in this booklet(see Arthritis Foundation booklets ‘Osteoarthritis’ and‘Rheumatoid Arthritis’).
PSORIATIC BOOKLET 12 PAGE.qxd 2010/03/16 02:41 PM Page 3
What is the cause? At present, the exact cause is unknown.
A particular combination of genes make some people morelikely to get psoriasis and psoriatic arthritis. Current researchsuggests that something (perhaps an infection) acts as a triggerin people who are susceptible to this type of arthritis becauseof their genetic make-up. No specific infection has been foundand it may be that a variety of injections (including bacteriathat live in patches of psoriasis) can trigger the disease. Figure 2. Symptoms of psoriatic arthritis: a. pitting and dis- Will my children develop psoriatic arthritis? Your children will be more likely than the next person to get psori-atic arthritis but the risk is still low.
Both psoriasis and psoriatic arthritis occur more frequently insome families than in others. Sometimes other diseases such
PSORIATIC BOOKLET 12 PAGE.qxd 2010/03/16 02:41 PM Page 4
as inflammation of the bowel (Crohn’s disease and ulcerativecolitis), stiffening of the spine (ankylosing spondylitis) andsevere eye inflammation (iritis or uveitis) also run in the samefamily. The link is genetic but the risk of passing it on is low. What links the skin and the joints in psoriatic arthritis? The link is probably genetic but fortunately many treatments helpthe skin and the joints at the same time.
Some people find that when their psoriasis is bad their arthri-tis is also bad and as one improves, so does the other. It is pos-sible that bacteria in the skin disease trigger the inflammationin the joints (see ‘What is the cause?’). Most people develop pso-riasis before the arthritis but about 1 in 10 develop the arthri-tis first.
Who can help? Treatment is given by a team of health workers (usaually a rheuma-tology team) including doctors, nurses, physiotherapists, occupa-tional therapists and podiatrists.The doctor (either your GP or a specialist) will normally be the first to diagnose your condition, and will probably also be the person who refers you to other members of the team and starts treatment with drugs. The other members of the health team play an important role in helping you to understand the disease, as well as monitoring the condition and providing treatment within their own specialist areas. Their advice and treatments are invaluable because tablets are not the only way of treating psoriatic arthritis. Although the roles of the rheumatology team members overlap, a general guide to their specialist areas is shown below: The nurse practitioner will provide information and guidance about your disease and the drugs you take but will also give advice and information relating to your home and personal situation. The physiotherapist will assist you with physical therapies (use of heat, cold, and other therapies to help your joints) and will advise on helpful exercises. It is important to maintain the mobility of your joints as well as maintaining the strength in your muscles. Exercise therapy is particularly important in people with spinal inflammation (spondylitis). The occupational therapist has an important role in advising
PSORIATIC BOOKLET 12 PAGE.qxd 2010/03/16 02:41 PM Page 5
you on how to protect your joints from further damage ands\he may give you splints to wear - particularly on your wristsand hands (see Figure 3). S\he will also assess whether equip-ment is needed to help you cope at home. Figure 3. A wrist splint The podiatrist (foot specialist) will assess your need for reg- ular foot care and whether specially made insoles will help you. S\he will also advise on footwear and where you can buy appropriate shoes. The hospital pharmacist will probably offer extra advice on the tablets prescribed. Many of the tablets used for psoriatic arthritis are also used in other forms of arthritis, particularly rheumatoid arthritis. This is because in both conditions the joints become inflamed and the tablets are used to control this inflammation. Information about the main types of tablets used is shown below. What are anti-inflammatory drugs? Anti-inflammatory drugs act by blocking the effects of the inflamma-tion which occurs in the lining of your joints.
They can be very effective in controlling the pain and stiffnessof arthritis. Usually you will feel a benefit within hours of tak-ing these drugs but the effect will only last for a few hours, sothe tablets have to be taken at regular intervals for the benefitto continue. Some people find that these tablets are of littlehelp, while others find that they help at first but the benefitbegins to wear off after a few weeks. In this situation it some-times helps to try a different anti-inflammatory drug
Examples of anti-inflammatory drugs
Diclofenac, ibuprofen, indometacin, naproxen, nabumetone,piroxicam
The main side-effect of the anti-inflammatory drugs is indiges-tion and, in some cases, the drugs can cause a stomach ulcer. For this reason doctors recommend taking these tablets withor after food. You must tell a health professional (preferably amember or the rheumatology team) if you get indigestion
PSORIATIC BOOKLET 12 PAGE.qxd 2010/03/16 02:41 PM Page 6
while taking these drugs as something can be done to help.
What are disease-modifying drugs? Disease-modifying drugs help by attacking the causes of the inflam-mation in the lining of the joints.
These drugs act quite differently from anti-inflammatorydrugs and hopefully will stop your arthritis from gettingworse. Unlike anti-inflammatory drugs it may be severalweeks before they start to have an effect on your joints. Therefore it is important to keep going with these tablets evenif you think they aren’t doing any good. Sometimes thesedrugs are given by injection because a suitable tablet is notavailable.
Disease-modifying drugs are normally used as a ‘second-line’treatment and the decision to use them will depend on a num-ber of factors including the effects of the anti-inflammatorydrugs, the activity of the arthritis and the likelihood of furtherjoint damage. Your doctor will discuss these factors with youbefore starting treatment. Examples of disease-modifying drugs Older drugs: chloroquine/hydroxychloroquine, ciclosporin, gold, methotrexate, penicillamine, sulfasalazine Newer drugs: adalimumab, anakrina, etanercept, infliximab
Anti-inflammatory drugs can be taken along with disease-modifying drugs. In fact, it is sometimes necessary to givemore than one disease-modifying drug, so you could end uptaking several tablets a day. Not surprisingly some people feelsick after all these tablets but there are ways of preventing this- you could try taking your tablet with a meal (unless yourdoctor advises you not to).
The side-effects of disease-modifying drugs are more complexthan with anti-inflammatory drugs. With almost all disease-modifying drugs you will need to have a regular blood testand, in some cases, a urine test. The blood test allows yourdoctor to monitor the effects of the drug on your disease, alsoto check that the drug is not causing problems with your bloodcount (the number of blood cells) or affecting your liver andkidneys. To help this monitoring a ‘shared-care’ card is pro-vided which is used to keep details of the drugs, their doses,and the results of blood tests. You should carry this card at alltimes.
PSORIATIC BOOKLET 12 PAGE.qxd 2010/03/16 02:41 PM Page 7
Will I need steroid treatments? Steroids are often recommended as an injection to the inflamed jointor where the tendon attaches to the bone.
In general, steroid tablets (such as prednisolone) are not usedfor psoriatic arthritis. However, small injections of steroid areoften recommended for joints which are particularly trouble-some and for the painful bony sites where ligaments and ten-dons become inflamed. What treatments will be used for the skin? Treatment is usually with ointments but if these don’t help you mayneed tablet treatment and light therapy.
Ointments and creams can be of five types:
• tar-based ointment and creams (it may not be obvious that
• dithranol-based ointments and creams (These can burn nor-
mal skin, so it is important to follow the instructions care-fully.)
• steroid-based ointments, creams and lotions
• vitamin D-like such as calcipotriol and tacalcitol
• vitamin A-like (retinoid) gels such as tazarotene.
If the creams and ointments do not help the psoriasis yourdoctor may suggest light therapy and\ or tablets such asretinoids (which are similar to vitamin A). Light therapyinvolves being exposed to high intensity ultraviolet light forshort periods and has to be carried out in a hospital.
Many of the disease-modifying drugs used for psoriatic arthri-tis will also help the skin disease. Similarly, some of the treat-ments for psoriasis may help the arthritis. For this reason der-matologists will often work together in treating you.
Treatments for nail psoriasis are usually less effective than theskin treatments. Nail blemishes are often very noticeable tothe person who suffers from them but fortunately much less soto other people. Some people use nail varnish to make the
PSORIATIC BOOKLET 12 PAGE.qxd 2010/03/16 02:41 PM Page 8
How much rest and exercise should I take? It is hard to generalize on this question - no two people are the same. Inflammation can cause generalized tiredness and you may find youneed to take more rests than usual. On the other hand, it is veryimportant to keep exercising the joints.
Inflammation can lead to muscle weakness and stiffness in thejoints. Exercise is important to help prevent this and keep thejoints functioning properly. You will need to find the rightbalance for yourself but remember not to neglect either rest orexercise when you are trying to help your disease.
Chronic pain can get you down and may cause stress, anxietyand depression. Counselling can help, and so can relaxationtechniques - these can be taught by a physiotherapist. Stress isnot the cause of psoriatic arthritis but can make it feel worse -so it will help if you can find ways of reducing and dealingwith stress. Are any special diets recommended? Many diets have been suggested for psoriatic arthritis but none havebeen found to be very effective.
A number or books recommend different diets for people witharthritis. However, some books contradict each other. Somemay even recommend stopping your tablets in order to try thediet. Don’t do this without discussing it with your doctor. Sometimes the diet can reduce the need to take tablets butunfortunately this is rare. Fish oils from marine (sea water)fish may reduce the amount of anti-inflammatory drugs need-ed to control joint inflammation and may therefore be worth atry.
If you are overweight, you need to follow a weight-reducingdiet because extra weight will add to the strain on your legjoints and back.
For more information, see Arthritis Foundation booklets ‘Dietand Arthritis’ and ‘Complemetary Therapies and Arthritis’.
PSORIATIC BOOKLET 12 PAGE.qxd 2010/03/16 02:41 PM Page 9
Should I give up work? The answer to this question depends on your arthritis, your age andyour job.
People who work - both in physical jobs and in offices - willhave difficulties if they develop arthritis, but the problem maynot be as serious as it first appears. Will this disease affect my sex life or my chances or having children? Your chances of having children will not be affected. Painful jointscan be a problem and interfere with your sex life but there are waysround this.
Psoriatic arthritis will not in itself affect your chances of hav-ing children or a successful pregnancy. For a woman whobecomes pregnant, the arthritis often improves during thepregnancy. However, the arthritis may worsen again after thechild has been born. It is worth remembering that lookingafter small babies is hard work and even harder if you havepainful joints. Would-be mothers with psoriatic arthritisshould therefore try to arrange plenty of help with childcare.
Some of the drug treatment given for psoriatic arthritis should be avoided when trying to start a family. For instance, sul- fasalazine can cause a low sperm count (this is not permanent) and you should not try for a baby if you or your partner are on methotrexate or have been using it in recent months. If you are considering starting a family you should discuss your drug treatment with your doctor.
Sexual intercourse may be painful, particularly for a womanwhose hips are affected. Using different positions can help. Itmay help to discuss this with a member of the rheumatologyteam. Will I need an operation? Operations are sometimes necessary to repair damaged tendons and,more rarely, to replace worn-out joints.
Operations are not often needed in psoriatic arthritis. Veryoccasionally a tendon may become damaged and need surgi-cal repair. Sometimes, after many years of disease, a jointworn out by inflammation is best treated by a replacementwith an artificial joint. There is no reason why this should be
PSORIATIC BOOKLET 12 PAGE.qxd 2010/03/16 02:41 PM Page 10
any more difficult in psoriatic arthritis than in any other typeof arthritis. However, if the psoriasis is bad in the skin aroundthe affected joint some surgeons like to give a course of antibi-otic tablets to help prevent infection. Sometimes psoriasis canoccur along the scar of the operation, but this can be treated inthe usual way. What will the future hold for me? Psoriatic arthritis can vary from a simple condition to a long-termproblem requiring complicated treatment.
Everyone is different. Therefore it is impossible to offer spe-cific advice on what you should expect. Most people with thiscondition will be on long-term treatment with anti-inflamma-tory and disease-modifying drugs. Generally, people withpsoriatic arthritis are less disabled than people with rheuma-toid arthritis, but their overall quality of life may be equallyaffected.
Butler University Health Services Allergy Injection(s) Consent / Policy Form Allergy Injection(s) Butler University Health Services will administer allergy shots to students who have the Required Information for the Administration of Allergen Immunotherapy Form, from their doctor, a signed consent form and serum. Students are seen for allergy injections only by appointment. Please see
PRESS RELEASE Wanbury enters Urinary infection antibiotic market with NDDS Nitrofur SR October 13, Mumbai: Wanbury Ltd, one of the fastest growing pharma companies in the domestic market, has launched its New Drug Delivery System (NDDS) product Nitrofur SR (Nitrofurantoin-100mg, sustained release) targeted at Urinary Tract Infections (UTI), for the first time in India. The m
 PSORIATIC BOOKLET 12 PAGE.qxd 2010/03/16 02:41 PM Page 1
What is in this booklet?
PSORIATIC BOOKLET 12 PAGE.qxd 2010/03/16 02:41 PM Page 1
What is in this booklet?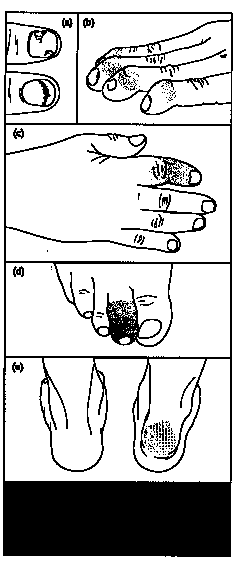 PSORIATIC BOOKLET 12 PAGE.qxd 2010/03/16 02:41 PM Page 3
What is the cause?
PSORIATIC BOOKLET 12 PAGE.qxd 2010/03/16 02:41 PM Page 3
What is the cause? PSORIATIC BOOKLET 12 PAGE.qxd 2010/03/16 02:41 PM Page 5
you on how to protect your joints from further damage ands\he may give you splints to wear - particularly on your wristsand hands (see Figure 3). S\he will also assess whether equip-ment is needed to help you cope at home.
PSORIATIC BOOKLET 12 PAGE.qxd 2010/03/16 02:41 PM Page 5
you on how to protect your joints from further damage ands\he may give you splints to wear - particularly on your wristsand hands (see Figure 3). S\he will also assess whether equip-ment is needed to help you cope at home.