Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Acr87.tmp
success in complex human diseases such as human im-munodeficiency virus.2 To determine whether such an
approach might be effective in ALS, we evaluated thecombination of two agents currently available for hu-
man use. Experimental administration of either mino-
cycline or creatine has been demonstrated to delay dis-ease onset and extend survival in transgenic mouse
Wenhua Zhang, MD, PhD, Malini Narayanan, MS, MD,
models of ALS.3–6 Given that these two compounds
act by different mechanisms of action, we evaluatedwhether the combination of minocycline with creatinemight result in additive neuroprotective effects in ALS
The known neuroprotective effects of minocycline and
mice. We report that the combination of minocycline
creatine in animal models of amyotrophic lateral sclerosis
and creatine results in an additive effect, delaying dis-
(ALS) led us to examine whether the combination of
ease onset, slowing progression, and delaying mortality. these agents would result in increased neuroprotection.
Because these two compounds are currently available
As previously reported, we confirmed in ALS mice that
for human use, their combined use may be evaluated
either minocycline or creatine treatment results in im- provement in motor performance and extended survival. We report that combination of minocycline and creatine resulted in additive neuroprotection, suggesting this to be Materials and Methods a novel potential strategy for the treatment of ALS. To our knowledge, this is the first report demonstrating ad-
Mice carrying the human SOD1G93A mutant gene were ob-
ditive neuroprotection of a combinatorial approach in a
tained from Jackson Laboratories (Bar Harbor, ME). Mice
mouse model of ALS. Adding relevancy to our findings,
were crossbred and genotyped as previously described.7 Mice
minocycline and creatine, are relatively safe, cross the
were fed a diet supplemented with 2% creatine beginning at
blood–brain barrier, and are currently available for hu-
3 weeks of age (courtesy of Dr R. Kaddurah-Daouk). Mino-
man evaluation.
cycline (22mg/kg body weight/day) was injected intraperito-
neally beginning at 4 weeks of age (Sigma, St. Louis, MO). Minocycline was prepared fresh in 0.9% saline daily. Themonotherapy and untreated groups were fed control diet or
Amyotrophic lateral sclerosis (ALS) is a chronic neuro-
injected with saline as appropriate in the same schedule asthe treated groups. Experiments were conducted in accor-
degenerative disease characterized by progressive motor
dance with protocols approved by the Harvard Medical
weakness resulting from selective motor neuron cell
death.1 Mortality is seen on the average 4 years after
The selection of 10 mice per group was determined from
disease onset. Proven therapeutic options are limited to
our previous experience evaluating minocycline in ALS
riluzole, which extends survival by an average of 3
mice.3 In that study, using 10 mice per group, we detected
months.1 It is therefore of utmost importance to de-
10% protection mediated by minocycline. Given the above-
velop novel and more effective therapeutics for this
mentioned information, as well as our hypothesis that the
universally fatal devastating disease. Because of the
combinatorial regimen would result in improved protection,
multifactorial downstream pathogenic pathways acti-
we decided to evaluate a group size of 10.
vated in ALS, improving therapeutic efficacy will de-pend on implementing a strategy addressing multiple
components of the pathogenesis. Combinatorial thera-
Motor strength and coordination were evaluated with a Ro-
peutics have been implemented with varying degrees of
tarod (Columbus Instruments, Columbus, OH), beginningat 10 weeks of age. Mice were evaluated at 5 and 15rpm. The time each mouse remained on the rod was registeredautomatically. If the mouse remained on the rod for 7 min-utes, the test was completed and scored as 7 minutes. Mice
From the Neuroapoptosis Laboratory, Department of Neurosurgery,
were tested weekly until they could no longer perform the
Brigham and Women’s Hospital, Harvard Medical School, Boston,
task. Two investigators performed the experiment, one eval-
uated Rotarod performance and was blinded to mice treat-
Received Jul 17, 2002, and in revised form Nov 5. Accepted for
ments (M.N.), and the other treated the mice (W.Z.). Onset and SurvivalDisease onset was defined as the first day that a mouse could
Address correspondence to Dr Friedlander, Neuroapoptosis Labora-
not remain on the Rotarod for 7 minutes at 15rpm. Mor-
tory, Department of Neurosurgery, Brigham and Women’s Hospi-
tality was scored as the age of death or the age when the
tal, Harvard Medical School, Boston, MA 02115. E-mail: rfriedlander@rics.bwh.harvard.edu
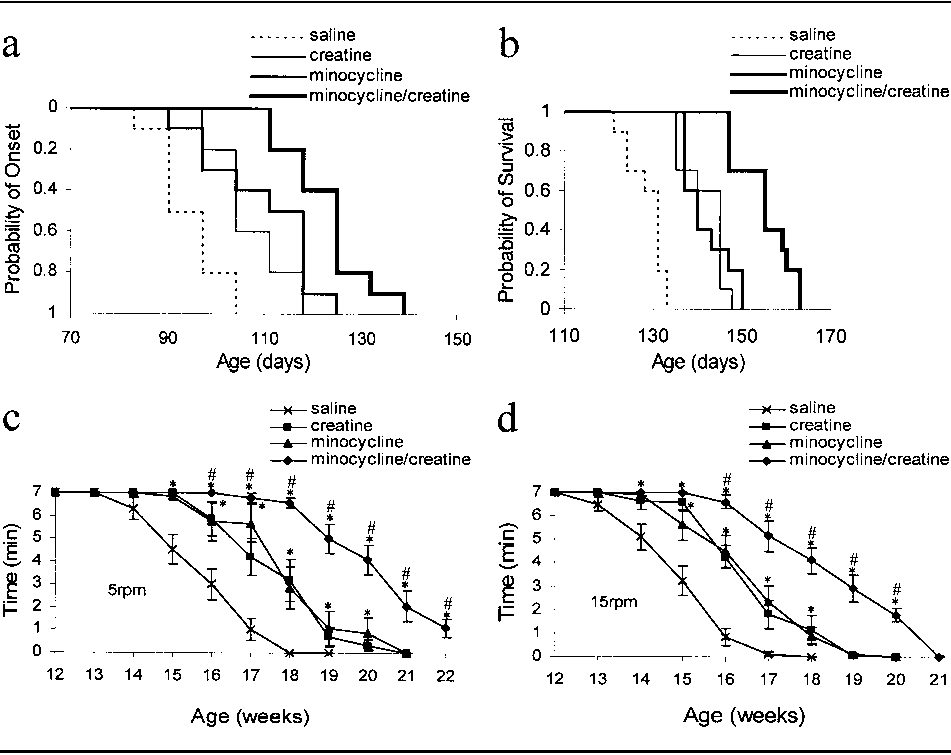
mouse was unable to right itself within 30 seconds. Statistical AnalysisThe findings were reported as the mean Ϯ standard devia-tion. Statistical comparisons between control group andtreated groups were performed using one-way analysis ofvariance. Results As previously reported, mutant SOD1G93A mice treated with either intraperitoneal injections of minocycline or 2% oral creatine demonstrated a significant delay of disease onset and increased survival as compared with mice fed unsupplemented diets and injected with saline (Table).3,4,5,6 Disease onset was delayed to 113 and 111 days, respectively, in the minocycline- and creatine-treated groups as compared with 94 days in the control group ( p Ͻ 0.05). Survival was similarly delayed in the minocycline and creatine groups to 142 Fig. Cumulative probability of onset of Rotarod deficits (a)
and 141 days, respectively, as compared with 126 days
and survival (b) in amyotrophic lateral sclerosis (ALS) mice.
in the control group ( p Ͻ 0.05). Minocycline-creatine
Survival was significantly prolonged and the onset of Rotarod
combination resulted in additive neuroprotection, with
deficit was significantly delayed in ALS mice treated with mi-
disease onset detected at 122 days and mortality at 157
nocycline and/or creatine when compared with saline-treatedtransgenic littermates. Combination of minocycline with creat-
days. The differences of onset and survival between the
ine significantly delayed onset and mortality as compared with
monotherapy groups and the minocycline-creatine
minocycline or creatine alone. Motor function was tested with
group were significantly different ( p Ͻ 0.05). Survival
the Rotarod at 5 (c) and 15rpm (d). Testing was terminated
was extended by 13%, 12%, and 25% in the minocy-
either when the mouse fell from the rod or at 7 minutes if the
cline, creatine, and minocycline-creatine groups, re-
mouse remained on the rod. Mice treated with the
spectively, as compared with the control group. minocycline-creatine combination performed significantly better
Kaplan–Meier curves of disease onset and survival as
than mice treated with either compound alone ([pound sign]
well as plots of Rotarod performance clearly demon-
p Ͻ 0.05). Mice treated with either minocycline or creatine
strate the additive protection of the minocycline-
performed significantly better than control mice ([asterisks] p
creatine combination (Fig). At the doses and schedule
Ͻ 0.05, n ϭ 10 per group).
tested, there were no significant differences in motorperformance or disease progression between the mino-
these abnormalities are interrelated, although a direct
cause and effect relationship cannot always be clearlydelineated. Therapeutic approaches targeting only one
Discussion
of the above-described abnormalities is likely to have
Successful combinatorial approaches rely on the use of
only a very limited impact on the progression of the
agents with different but complementary mechanisms
disease. Similar to what has been successfully executed
of action. This approach is of particular importance
in cancer and human immunodeficiency virus, a com-
when treating diseases with complex and multiple
bination of drugs targeting different components of the
pathologic abnormalities. A broad variety of cellular
particular pathophysiology of the disease will result in
abnormalities have been described in human specimens
enhanced effects as compared with monotherapeutic
and mouse models of ALS. Broadly, documented ab-
approaches.2 Using the incremental knowledge we have
normalities in ALS include apoptotic, bioenergetic, ex-
acquired regarding the mechanisms of pathogenesis in
citotoxic, and mitochondrial pathways.1,3,4,7–9 Many of
ALS, we are in the position to design rational thera-
Table. Onset of Motor Deficits and Mortality of ALS Mice Treated with Minocycline and/or Creatine (mean Ϯ SD)
ap Ͻ 0.05 compared with saline group.
bp Ͻ 0.05 compared with minocycline and with creatine group. ALS ϭ amyotrophic lateral sclerosis; SD ϭ standard deviation.
peutics, targeting different components of this disease.
studies have been done in single therapy of creatine4
The result of these experiments is the first demonstra-
and minocycline5 in mSOD1G93A transgenic mice.
tion of the efficacy of this approach in ALS. Further-
Klivenyi and colleagues demonstrated a remarkable in-
more, many patients with ALS are likely taking com-
hibition of motor neuron cell loss in creatine-treated
binations of medications, with no objective evidence of
ALS mice as compared with control ALS littermate
any benefit, and exposing themselves to potential for
mice.4 Furthermore, Van den Bosch and colleagues re-
harmful interactions or additive side effects.
ported decreased microglial activation in spinal cord.5
Minocycline is a second-generation tetracycline, cur-
Synergistic protection of motor neurons could likely
rently used in the treatment of certain infections, acne,
explain the additive neuroprotection detected in this
and rheumatoid arthritis. Minocycline is used as a
study using minocycline and creatine.
chronic medication in the latter two diseases. Cur-
For the first time to our knowledge, we report effec-
rently, the mode of action of minocycline appears to be
tive additive neuroprotection in a therapeutic trial us-
multifactorial. We recently have demonstrated that a
ing ALS mice. Note that the ability to rationally design
direct action of minocycline is inhibition of mitochon-
such studies has depended on incremental understand-
drial permeability transition–mediated release of cyto-
ing of the mechanisms of disease progression in ALS,
chrome c.3 Given that release of cytochrome c is a crit-
as well as the mechanisms of action of minocycline and
ical component of the apoptotic cascade, inhibition
creatine. Even greater neuroprotection than that dem-
of cytochrome c release results in inhibition of cell
onstrated from the minocycline-creatine combination
death. Additional activities have been associated with
might result from including additional compounds
minocycline-mediated neuroprotection including inhi-
with complementary mechanisms of action. In light of
bition of reactive microgliosis, of caspase-1, caspase-3,
the above described results, the relative safety record of
and nitric oxide synthase transcriptional upregulation
minocycline and creatine, and their ability to cross the
and of p38 MAPK activation.9–13 Whether any of
blood–brain barrier, their combined use may be evalu-
these properties of minocycline are direct or reactive in
nature remains to be elucidated. In addition to ALS,minocycline thus far has been demonstrated to be ef-fective in experimental models of stroke, Huntington’s
This work was supported by grants from the NINDS (NS41635
disease, Parkinson’s disease, and trauma.10–12,14
Creatine is an amino acid endogenously produced
from glycine, methionine, and arginine in the liver,kidney, and pancreas. It has remarkable neuroprotec-
References
tive qualities in models of ALS, traumatic brain injury,
1. Rowland LP, Shneider NA. Amyotrophic lateral sclerosis.
Huntington’s disease, and Parkinson’s disease.4,15–17
2. Temesgen Z, Wright AJ. Antiretrovirals. Mayo Clin Proc 1999;
Currently, the mechanism of creatine-mediated neuro-
protection is not well understood. Creatine kinase
3. Zhu S, Stavrovskaya IG, Drozda M, et al. Minocycline inhibits
along with its substrates creatine and phosphocreatine
cytochrome c release and delays progression of amyotrophic lat-
constitute key components of cellular bioenergetic
eral sclerosis in mice. Nature 2002;417:74 –78.
pathways.4 The mechanistic basis for the neuroprotec-
4. Klivenyi P, Ferrante RJ, Matthews RT, et al. Neuroprotective
effects of creatine in a transgenic animal model of amyotrophic
tive effects of creatine may involve alterations of the
lateral sclerosis. Nat Med 1999;5:347–350.
insult-induced depletion of cellular ATP, because
5. Van Den Bosch L, Tilkin P, Lemmens G, Robberecht W. Mi-
chronic ingestion of creatine results in increased brain
nocycline delays disease onset and mortality in a transgenic
levels of phosphocreatine. To this regard, creatine pro-
model of ALS. Neuroreport 2002;13:1067–1070.
tects mitochondrial creatine kinase activity against
6. Kriz J NM, Nguyen M, Julien J. Minocycline slows disease pro-
gression in a mouse model of amytrophic lateral sclerosis. Neu-
peroxynitrite-induced inactivation, which may play a
role in tissue damage in ALS.18 Most recently, direct
7. Gurney ME, Pu H, Chiu AY, et al. Motor neuron degeneration
antioxidant properties of creatine have been described
in mice that express a human Cu,Zn superoxide dismutase mu-
that may be relevant to explain some of its neuropro-
tation. Science 1994;264:1772–1775.
tective effects.19 Creatine has been evaluated in human
8. Friedlander RM, Brown RH, Gagliardini V, et al. Inhibition of
ICE slows ALS in mice. Nature 1997;388:31.
ALS trials. Preliminary results demonstrated that crea-
9. Martin LJ. Neuronal death in amyotrophic lateral sclerosis is
tine supplementation temporarily increases maximal
apoptosis: possible contribution of a programmed cell death
mechanism. J Neuropathol Exp Neurol 1999;58:459 – 471.
This study does not address neuropathological
10. Yrjanheikki J, Keinanen R, Pellikka M, et al. Tetracyclines in-
changes in combined therapy compared with mono-
hibit microglial activation and are neuroprotective in global brainischemia. Proc Natl Acad Sci USA 1998;95:15769 –15774.
therapy. However, neuropathological studies may help
11. Chen M, Ona VO, Li M, et al. Minocycline inhibits caspase-1
elucidate the mechanism of additive neuroprotection
and caspase-3 expression and delays mortality in a transgenic
using minocycline and creatine. Neuropathological
mouse model of Huntington disease. Nat Med 2000;6:797– 801.
12. Du Y, Ma Z, Lin S, et al. Minocycline prevents nigrostriatal do-
phagia in 8 patients, also were observed among our
paminergic neurodegeneration in the MPTP model of Parkin-
LEMS population. More than one prereferral oculobul-
son’s disease. Proc Natl Acad Sci USA 2001;98:14669 –14674. bar feature occurred in 13 of our LEMS patients. Prere-
13. Almer G, Vukosavic S, Romero N, Przedborski S. Inducible
nitric oxide synthase up-regulation in a transgenic mouse model
ferral diagnostic considerations included myasthenia gra-
of familial amyotrophic lateral sclerosis. J Neurochem 1999;72:
vis, myopathies, and psychiatric disorders. These findings suggest that these atypical characteristics served to dis-
14. Sanchez Mejia RO, Ona VO, Li M, Friedlander RM. Minocy-
suade some colleagues from a diagnosis of LEMS. Thus,
cline reduces traumatic brain injury-mediated caspase-1 activa-
the presence of oculobulbar symptoms and signs cannot
tion, tissue damage, and neurological dysfunction. Neurosur-
be used to exclude LEMS from the differential diagnosis.
gery 2001;48:1393–1399; discussion, 1399 –1401.
15. Sullivan PG, Geiger JD, Mattson MP, Scheff SW. Dietary sup-
plement creatine protects against traumatic brain injury. AnnNeurol 2000;48:723–729.
16. Ferrante RJ, Andreassen OA, Jenkins BG, et al. Neuroprotec-
tive effects of creatine in a transgenic mouse model of Hunting-
The Lambert–Eaton myasthenic syndrome (LEMS) is
ton’s disease. J Neurosci 2000;20:4389 – 4397.
an autoimmune disorder of neuromuscular transmis-
17. Matthews RT, Ferrante RJ, Klivenyi P, et al. Creatine and cy-
sion.1–3 Typically when LEMS is related to a malig-
clocreatine attenuate MPTP neurotoxicity. Exp Neurol 1999;157:142–149.
nancy, it is almost always a small cell lung cancer
18. Wendt S, Dedeoglu A, Speer O, et al. Reduced creatine kinase
(SCLC). Although LEMS is sometimes associated with
activity in transgenic amyotrophic lateral sclerosis mice. Free
other neoplasms, 15% of patients with other SCLC-
19. Lawler JM, Barnes WS, Wu G, et al. Direct antioxidant prop-
related autoimmune disorders have a coexisting, unre-
erties of creatine. Biochem Biophys Res Commun 2002;290:
lated, and often obvious neoplasm.4–13 When there is
no paraneoplastic mechanism identified, LEMS usually
20. Mazzini L, Balzarini C, Colombo R, et al. Effects of creatine
has a primary autoimmune basis sometimes associated
supplementation on exercise performance and muscularstrength in amyotrophic lateral sclerosis: preliminary results.
with other immunological disorders.7,10 The neuro-
physiological characteristics of LEMS represent theclinical prototype of a presynaptic neuromusculartransmission disorder.1,4-6 The voltage-gated calciumchannel of motor nerve terminals is the primary site ofimmune attack.3,8,9
Classically, LEMS presents with fatigability, proxi-
mal weakness, hyporeflexia or areflexia of the muscle
stretch reflexes, and cholinergic dysautonomia.4–7,14Oculobulbar symptoms are reported to be less com-
mon and mild and therefore have not received much
Ted M. Burns, MD,1 James A. Russell, MD,1
attention.6,7,14 The diagnosis of LEMS is sometimes
quite challenging. This is because of its relative rarity,
the nonspecificity of symptoms with fatigue as a pri-mary clinical complaint, often the generally mild na-ture of objective weakness, and because the symptoms
Oculobulbar symptoms and/or signs were present in 18
of dysautonomia are often overlooked. Last, the pro-
of 23 (78%) of Lambert–Eaton myasthenic syndrome (LEMS) patients evaluated at the Lahey Clinic (Table).
tean clinical presentations of LEMS are not always ap-
Sixty-five percent (15 of 23) of our patients had ptosis
preciated. Because of the therapeutic importance inher-
and/or diplopia, each present in 11 individuals. Bulbar
ent in the early recognition of LEMS, it is incumbent
signs and symptoms, including dysarthria in 10 and dys-
on the neurologist to be aware of these variable clinicalpresentations. Because it is our clinical experience thatLEMS may be underrecognized and its diagnosis is of-ten delayed, we have reviewed our series of 23 LEMS
From the 1Department of Neurology, Lahey Clinic, Burlington,MA, and the 2Department of Neurology, Mayo Clinic, Rochester,
patients diagnosed at the Lahey Clinic. These data
demonstrate that oculobulbar involvement, so typical
Received Jun 14, 2002, and in revised form Nov 11. Accepted for
of myasthenia gravis (MG), is also a more common
clinical finding of LEMS than is emphasized in theclassic teaching of this entity. Recognition of this ob-servation may enhance an earlier diagnosis of the
Address correspondence to Dr Burns, Lahey Clinic, 41 Mall Road,Burlington, MA 01805. E-mail: tmb8r@virginia.edu
SV-Bundessiegerzuchtschau Gebrauchshundeklasse RÜDEN VA 1 VA= vorzüglich Auslese; V = vorzüglich; SG = sehr gut; G = gut; U = ungenügend; EZ = entschuldigt zurückgezogenT1 = läßt nicht ab, ohne Bew. TSB; T2 = TSB vorhanden; T3 = TSB nicht genügend; T4 = abgebrochen wegen mangelnder Führigkeit Verein für Deutsche Schäferhunde (SV) e.V. - EDV Sonntag, 7. September 2003 17:02:4
HORIZON HEALTH PULSE Hak Ko, MD Residents of Horizon Village now have another opportunity to help turn theirlives around while staying at the Village: a GED program available throughNiagara/Orleans BOCES Continuing Education. “The GED program, which is funded by Niagara County Social Services, is designed to helpour residents become less dependent on social services and re-enter so
 Statistical AnalysisThe findings were reported as the mean Ϯ standard devia-tion. Statistical comparisons between control group andtreated groups were performed using one-way analysis ofvariance.
Statistical AnalysisThe findings were reported as the mean Ϯ standard devia-tion. Statistical comparisons between control group andtreated groups were performed using one-way analysis ofvariance.