Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Bacdot
STOP TB LVIV BACDOT Study Impact of the new bacteriological procedures and supervised therapy on the outcome of patients with newly diagnosed, smear-positive pulmonary TB in The BACDOT Study
Thomas Bodmer and Jean-Pierre Zellweger for the ‚STOP TB LVIV’ Study Group
STOP TB LVIV BACDOT Study Executive Summary Impact of the new bacteriological procedures and supervised therapy on the outcome of patients with newly diagnosed, smear-positive pulmonary TB in Lviv/UA Background: The results of the Sychiv pilot study revealed that almost 40% of newly diagnosed pulmonary tuberculosis (TB) patients were infected with drug-resistant Mycobacterium tuberculosis (MTB). Almost half of these cases were multidrug-resistant MTB (MDR-TB). Patients who are infected with such strains generally do not respond favourably to the standard drug regimen recommended by WHO. Inadequate drug therapy will result in treatment failures and continued transmission of drug-resistant strains. Therefore it is of the utmost importance to rapidly identify these patients and to treat them as soon as possible according to the results of drug susceptibility testing (DST).
Recently, several improvements in the management of tuberculosis patients in Sychiv were implemented, such as the introduction of the Bactec 960 technology including drug sensitivity testing in liquid medium, training of the staff in improved methods for smear examination, electronic registration of samples and results, improvement of the coordination between laboratory and clinicians, training of clinicians and health-care workers in the DOTS strategy, and hiring of TB nurses for the supervision of the ambulatory phase of treatment of patients. It is to be expected that these changes will have an impact on the outcome of treatment, first of patients with drug-sensitive tuberculosis, then also on patients with drug resistance.
Study goals:
1. to evaluate the impact of new procedures at the local laboratory in Sychiv on the
management of patients with newly diagnosed pulmonary TB
2. to assess the drug sensitivity patterns of patients with newly diagnosed pulmonary TB 3. to assess the outcome of patients with newly diagnosed, drug-sensitive pulmonary
tuberculosis under appropriate follow-up conditions (DOT)
4. to assess the conditions of and obstacles to an optimal management of patients with
tuberculosis during the ambulatory phase of treatment
Relevance of the study: The study supports the consolidation of the new Core Laboratory at Sykhiv hospital and prepares the introduction of molecular testing for drug-resistant MTB. Data on the local drug resistance rates of MTB and risk factors that are associated with drug resistance will be generated. In addition, the effect of the rapid diagnosis of MDR-TB on patient management will be studied, and, importantly, some elements of WHO’s DOTS strategy will be implemented, and the results compared to the current situation. STOP TB LVIV BACDOT Study Study description Patients and methods: A total of 100 consecutive adult patients with newly diagnosed sputum smear-positive pulmonary TB from the city of Lviv/UA will be included in the study. In total, 4 sputum specimens per patient (2 specimens initially; one further specimen after 2 and 5 months of treatment,) will be submitted to the Core Laboratory at Sykhiv hospital and processed according to the new laboratory algorithm. Patients will be categorized according to the results of drug sensitivity testing (RIF-susceptible or RIF-resistant MTB) and treated accordingly, with pre-defined drug regimens. In addition, after release from the hospital, directly observed therapy (DOT) will be given to patients with RIF-susceptible TB by study nurses who report to the local study coordinator. The outcome data of the study group will be compared to the overall outcome data as the reference. Conditions for inclusion:
1. Patients with newly diagnosed smear-positive pulmonary tuberculosis
2. Strains sensitive to the first-line drugs or isoniazid resistance only (according to the
4. Agreeeing to be included in a register and followed until the end of treatment,
including daily supervised intake of drugs
5. Cases with resistance other than isoniazid only (in particular rifampicin resistance and
MDR-TB) will be excluded from the cohort but treated according to the local guidelines.
Outcomes:
1. Delay between the first medical examination and the results of
2. Proportion of drug-sensitive patients among all newly diagnosed pulmonary TB
3. Duration of hospitalization (for drug-sensitive cases only)
5. Outcome of treatment by WHO category (cure, treatment completion, failure, death,
STOP TB LVIV BACDOT Study Study goals:
1. to evaluate the impact of new procedures at the local laboratory in Sychiv on the
management of patients with newly diagnosed pulmonary TB
2. to assess the drug sensitivity patterns of patients with newly diagnosed pulmonary TB 3. to assess the outcome of patients with newly diagnosed, drug-sensitive pulmonary
tuberculosis under appropriate follow-up conditions (DOT)
4. to assess the conditions of and obstacles to an optimal management of patients with
tuberculosis during the ambulatory phase of treatment
Local study coordinator
The realisation of the BACDOT study will be coordinated and supervised locally by the local study coordinator Dr. Sinowij Nakonechnyi, deputy chief of Sykhiv hospital. His duties and responsibilities as a BACDOT local study coordinator are described in a separate document (see BACDOT Study Coordinator).
The study coordinator will be supported by a personal assistant for data collection, translation and communication. Martha Nakonechna was appointed assistant to the study coordinator. Her duties and responsibilities as an assistant to the BACDOT local study coordinator are described in a separate document (see BACDOT Study Coordinator).
The coordinates of Martha Nakonechna are:
STOP TB LVIV BACDOT Study Patients and methods
This section describes the phases of the BACDOT study.
Phase 0, Recruitment of study patients
Patients with a first episode of sputum smear-positive pulmonary tuberculosis (TB) who live in the City of Lviv are eligible. The recruitment procedure is summarized below. Overall, 10 to 15 cases per month of newly diagnosed patients with pulmonary TB from the city of Lviv are to be expected, i.e. recruitment of 100 patients may take between 7 and 10 months.
Figure 1: Recruitment of study patients Recruitment of patients Comments
General lab procedure (in Sykhiv) consists in
Study lab procedures (in Sykhiv) consists in
the signing of the informed consent form
the completion of the study questionnaire
Initial therapy of all study pts. consists in HREZ
Therapy will be adapted according to the results of drug susceptibility testing (DST):
RIF-resistant Mtb: individualized scheme
Pts. with RIF-sensitive TB (a; b) are eligible for DOT
Pts. with MDR TB (c) are NOT eligible for DOT
Sputum will be obtained from each patient and submitted to the central TB laboratory in Sykhiv. There, sputum specimens are processed upon receipt (NALC decontamination; high-performance centrifugation; fluorescence microscopy; both Bactec® MGIT 960 liquid and solid culture), and the microscopy results are reported to the attending physician and the local study coordinator.
Patients with a first episode of sputum smear-positive pulmonary TB who live in the City of Lviv are eligible, but definitive enrolment requires that patients give informed consent to be part of the study and complete the study questionnaire. Definitive enrolment is authorized by the local study coordinator who is responsible for the correct patient selection and enrolment procedure and the completeness of the study data.
STOP TB LVIV BACDOT Study Phase 1, Hospitalization and intensive phase drug therapy
All study patients will be hospitalized and intensive phase drug therapy (intensive phase; 0 to 8 weeks) will be initiated with HREZ according to the WHO recommendations (see figure 2).
Figure 2: Synopsis of the BACDOT Study Synopsis of the BACDOT Study Outcomes
Track A: pan-sensitive MTB; Track B: INH-resistant or INH-/SM-resistant MTB
Detection of RIF-resistant MTB
The first sputum sediment of each study patient will be cultured locally using the Bactec® MGIT 960 system.
Patients will be categorized into RIF-susceptible and RIF-resistant TB on the basis of the drug sensitivity testing results.
In Sykhiv the reports are forwarded to the attending physician by the local study coordinator. The delay between request of the examination and transmission to the attending physician will be recorded in the study files. The attending physician is responsible for adherence to, and documentation of, the study guidelines for subsequent categorization of the patients and the adaptation of drug regimens when indicated (see figure 2 and tab 3).
Drug-susceptibility testing
The RIF resistance will be demonstated by drug-susceptibility testing (DST) of cultured Mycobacterium tuberculosis by the Bactec® MGIT 960 system. The results should be available by the end of the intensive phase, i.e. within two months after initiation of therapy. DST results will guide the therapeutic decisions with regard to the continuation phase in cases of RIF-susceptible, mono- or poly-resistant MTB (see figure 2).
STOP TB LVIV BACDOT Study Standardised treatment regimens
Figure 2 gives a synopsis of the diverse treatment tracks of the BACDOT study. Tracks are based on the results of the detection of RIF resistance, conventional DST and the HIV status of the patient.
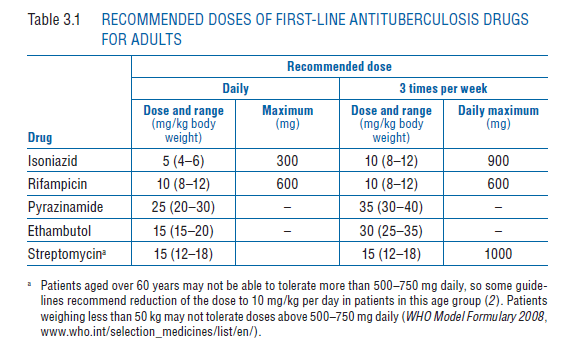
All study patients will be hospitalized and intensive phase drug therapy (intensive phase; 0 to 8 weeks) will be initiated according to the WHO recommendations with Isoniazid (INH; H), Rifampicin (RIF; R), Pyrazinamide (PZA; Z), and Ethambutol (EMB; E). Recommended doses for adults are given in table 1.
Table 1: Recommended doses of first-line anti-tuberculosis drugs. STOP TB LVIV BACDOT Study BACDOT treatment tracks
Patients with confirmed (on the basis of the DST results) RIF-susceptible TB are eligible for ambulatory directly observed therapy (DOT). All treatment will be given on a daily basis. Individual drug regimens are adapted according to the results of the DST (see tracks), and the patients will be discharged from the hospital under directly supervised treatment. Below, the most frequent therapeutic situations and their respective standardised drug regimens (treatment tracks A, B and C) are defined. More complex therapeutic situations can be discussed with the Study Coordinator and the Swiss partners.
Track A: pan-sensitive MTB (expected: 60% of study population)
After completion of the intensive phase of two months HREZ, patients with pan-sensitive MTB will receive a daily, supervised therapy with HR for an additional 4 months, i.e. for a total treatment period of 6 months. Whenever possible, this period of treatment should be organized on an ambulatory basis.
Track B: INH-resistant or INH-/SM-resistant MTB (expected: 20% of study population)
After completion of the intensive phase of two months HREZ, patients with INH-resistant MTB (but R-sensitive) will receive a daily, supervised therapy with RZE for an additional 4 months, i.e. for a total treatment period of 6 months. Whenever possible, the treatment should be organized on an ambulatory basis
Track C: MDR TB (expected: 20% of study population)
Patients with RIF-resistant MTB (on the basis of the Bactec 960 test) should be considered MDR TB patients until proven otherwise. These patients are excluded from the study and treated with a cat IV regimen according to the local and WHO Guidelines. A fluoro-quinolone (FQ), preferably levofloxacin (LVX), an injectable drug amikacin (AMK) or kanamycine (K) and one second-line drug are added to the HREZ treatment regimen until the results of the targeted DST become available. Then, individualised drug therapy is initiated on the basis of the DST results. Such patients will be treated according to the existing guidelines for MDR TB treatment, unless alternative MDR TB therapy, such as DOTS plus, seems appropriate to the local study coordinator.
Weight <50 kg Weight >50 kg Table 2: Recommended doses for Levofloxacin and Amikacin. Patients with confirmed RIF-resistant TB (track C; on the basis of the phenotypic DST results) are not eligible for the BACDOT study. STOP TB LVIV BACDOT Study Phase 2, Continuation phase, ambulatory drug therapy
The organisation of the drug delivery must be clarified prior to discharging a patient from the hospital. The direct contact between the patient and the community nurse in charge of the surveillance of the ambulatory phase will generally be established during the patient’s hospitalisation. In some cases, facilities for daily clinic visits might be necessary and require consideration (for instance bus tickets).
Following discharge from the hospital, the patients with confirmed RIF-susceptible pulmonary TB will be treated on an outpatient basis, under full supervision of drug intake, until the completion of the treatment. As the usual duration of hospitalization is 2 months or more (intensive phase of treatment with 4 drugs), we can assume that the patients under DOT will receive only isoniazid and rifampicin in the continuation phase.
The drugs will be given at least 5 days per week (ideally 6 days) under supervision, by means of the patient visiting the TB dispensary, a local clinic, or a GP, or by a home visit of a community nurse to the patient’s home or place of work.
The procedure for tracing patients in case of default should be decided in advance. Both the patient and the community nurse should be able to communicate with each other.
The person in charge of notifying the outcome of treatment (and responsible for action in case of default) should be designated in advance; this is the responsibility of the local study coordinator.
In case of transfer of a patient from the Sychiv Hospital to a sanatorium, the study coordinator will ensure the transmission of all medical information to the new place of treatment and the collection of data for the study files.
STOP TB LVIV BACDOT Study Assessing the treatment response
Note: If a patient is found to harbour a multidrug-resistant strain of MTB at any time during therapy, treatment is declared failure and the patient is re-registered and should be referred to a MDR-TB treatment programme.
a Omit if patient was smear-negative at the start of treatment and at two months. b Smear- or culture-positivity at the fifth month or later (or detection of MDR TB at any point) is defined as treatment failure
and necessitates re-registration and change of treatment.
Figure 3: Sputum monitoring by smear microscopy in new pulmonary TB patients
Additional sputum monitoring is needed for new patients whose sputum smear is positive at the end of the intensive phase:
1. In new patients, if the specimen obtained at the end of the intensive phase (month 2*)
is smear-positive, sputum smear microscopy should be obtained at the end of the third month.
* Sputum should be collected when the patient is given the last dose of the intensive-
2. In new patients, if the specimen obtained at the end of month 3 is smear-positive,
sputum culture and drug susceptibility testing (DST) should be performed.
A positive sputum smear at the end of the intensive phase may indicate any of the following:
• the initial phase of therapy was poorly supervised and patient adherence was poor; • poor quality of anti-TB drugs; • doses of anti-TB drugs are below the recommended range; • resolution is slow because the patient had extensive cavitation and a heavy initial
• there are co-morbid conditions that interfere either with adherence or with response; • the patient may have drug-resistant MTB that is not responding to first-line treatment; • non-viable bacteria remain visible by microscopy.
STOP TB LVIV BACDOT Study Definitions of treatment outcomes
The definitions below are based on the up-dated treatment of tuberculosis guidelines1 recently published by WHO.
Definition a
A patient whose sputum smear or culture was positive at the beginning of the treatment but who was smear- or culture-negative in the last month of treatment and on at least one previous occasion.
Treatment completed A patient who completed treatment but who does not have a negative
sputum smear or culture result in the last month of treatment and on at least one previous occasion. b
A patient whose sputum smear or culture is positive at 5 months or later during treatment. Also included in this definition are patients found to harbour a multidrug-resistant (MDR) strain at any point of time during the treatment, whether they are smear-negative or -positive.
A patient who dies for any reason during the course of treatment.
A patient whose treatment was interrupted for 2 consecutive months or more.
A patient who has been transferred to another recording and reporting unit and whose treatment outcome is unknown.
A sum of cured and completed treatment. c
Table 3: Definitions of treatment outcomes
a These definitions apply to pulmonary smear-positive and smear-negative patients. Outcome
of patients with extra-pulmonary disease needs to be evaluated separately.
b The sputum examination may not have been done or the testing results may not be
c For smear- or culture-positive patients only.
1 WHO. Treatment of tuberculosis guidelines; 4th edition, 2010
STOP TB LVIV BACDOT Study Table 4: Suggested standardized drug regimens
Estimates are based on the results of the STOP TB LVIV Pilot Study2. Suggested drug regimens follow published WHO guidelines3.
Patients with pan-susceptible tuberculosis Resistant to Proportion Drug regimen Min. duration Comments Patients with rifampin-susceptible, mono- or poly-resistant tuberculosis Resistant to Proportion Drug regimen Min. duration Comments
plus an injectable agent for the first 2-3 months
Patients with rifampin-resistant tuberculosis Resistant to Proportion Drug regimen Min. duration Comments
INH (H), Isoniazid; RIF (R), Rifampin; PZA (Z), Pyrazinamide; EMB (E), Ethambutol; SM (S), Streptomycin; FQ, Fluoroquinolone
2 Bodmer T., et al. Drug resistance of Mycobacterium tuberculosis in patients with new pulmonary tuberculosis in Lviv/UA (abstract). IUATLD 2009, Dubrovnik, CRO. 3 WHO emergency update 2008. Guidelines for the programmatic management of drug-resistant tuberculosis.
Ley de Procedimiento Administrativo, de 17 de julio de 1958 Esta Ley ha sido derogada por la Ley 6/1997, de 14 de Abril, de Organización y Funcionamiento de la Administración General del Estado. No obstante, los artículos que se transcriben conservan su vigencia, aunque con rango reglamentario, en virtud de la disposición derogatoria única de dicha disposición. La Ley de 19 de octu
MEDICAL HISTORY Name Birth date Please circle any of the following which you have or have had in the past Do you require antibiotics before dental treatment? Y N PRE-MED DOSEAGE Heart Conditions (Murmur, Rheumatic heart disease, Congenital defect, Mitral Valve Prolapse, Coronary Pregnant or breast-feeding currently (Women only) artery disease, Irregular heart beat, Co
 STOP TB LVIV BACDOT Study
STOP TB LVIV BACDOT Study 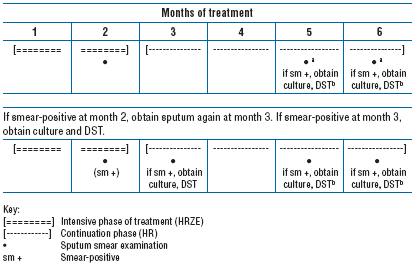 STOP TB LVIV BACDOT Study
STOP TB LVIV BACDOT Study