Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
15146_layout.fm
Prevention of dislocation of the hip in children with cerebral palsy
THE FIRST TEN YEARS OF A POPULATION-BASED PREVENTION PROGRAMME
G. Hägglund, In 1994, a register for cerebral palsy and a health-care programme were started in southern S. Andersson, Sweden with the aim of preventing dislocation of the hip in children with cerebral palsy. It H. Düppe, involved all children with cerebral palsy born in 1992 or later. H. Lauge-Pedersen, None of the 206 affected children born between 1992 and 1997 has developed a E. Nordmark, dislocation following the introduction of the prevention programme. Another 48 children L. Westbom moved into the area and none developed any further dislocation. Of the 251 children with cerebral palsy, aged between five and 11 years, living in the area on January 1, 2003, only two had a dislocated hip. One boy had moved into the area at age of nine with a dislocation and a girl whose parents chose not to participate in the programme developed bilateral dislocation. One boy, whose condition was considered to be too poor for preventative surgery, developed a painful dislocation of the hip at the age of five years and died three years later. Eight of 103 children in a control group, consisting of all children with cerebral palsy living in the area between 1994 and 2002, and born between 1990 and 1991, developed a dislocation of the hip before the age of six years. The decreased incidence of dislocation after the introduction of the prevention programme was significant (p < 0.001). Dislocation of the hip in cerebral palsy remains a serious problem, and prevention is important. Our screening programme and early intervention when lateral displacement of the femoral head was detected appear to be successful.
Children with cerebral palsy have an increased
Patients and Methods
risk of lateral displacement of the femoral
In 1994, a cerebral palsy register and health-
head, leading in some cases to dislocation. The
care programme for children with cerebral
reported incidence of lateral displacement or
palsy was started in southern Sweden involving
dislocation is related to the severity of the con-
all children born with cerebral palsy in the area
dition and varies between 7% in ambulatory
since 1990. The condition was defined as “an
children and 60% in those with total-body
involvement.1,2 However, no population-based
progressive, but often changing, motor impair-
NeuropaediatricianDepartment of Paediatrics
ment syndromes secondary to lesions or anom-
alies of the brain arising in the early stages of
results in significant morbidity in terms of
development”.11 Only children who were alive
pain,3-5 contractures, problems with sitting,
at two years of age and had their cerebral
Orthopaedic SurgeonDepartment of Orthopaedics
standing or walking,6 fractures,7,8 skin ulcera-
lesion before that time were included. The sub-
tion and difficulty with perineal care,6,8 pelvic
type of cerebral palsy was determined after the
fourth birthday according to the method of
Correspondence should be sent to Dr G. Hägglund.
The first suggestion that dislocation in cere-
function was classified according to the classi-
2005 British Editorial Society of Bone and
nearly 50 years ago.10 We initiated a popula-
fication system (GMFCS) of Palisano et al13
tion-based prevention programme for chil-
which is an age-related five-level system in
which level I is the least and level V the most
preventing dislocation of the hip by early
J Bone Joint Surg [Br] 2005;87-B:95-101.
detection and intervention. We now describe
The study area has a population of 1.3 mil-
and analyse the results of the first ten years of
lion. The total population of children born in
Accepted after revision 25 May 2004
1990 and later were systematically reviewed in
G. HÄGGLUND, S. ANDERSSON, H. DÜPPE, H. LAUGE-PEDERSEN, E. NORDMARK, L. WESTBOM
Table I. The gross motor function classification system (GMFCS).13 The levels represent the highest level of mobility that a child is expected to achieve between six and 12 years of age
Walks without restrictions; limitations in more advanced gross motor skills
Walks without assistive devices; limitations walking outdoors and in the community
Walks with assistive devices; limitations walking outdoors and in the community
Self-mobility with limitations; children are transported or use power mobility outdoors and in the community
Self-mobility is severely limited even with the use of assistive technology
Table II. Subdiagnosis and GMFCS* level in 103 children with cere-
In the present study children born between 1990 and
bral palsy born between 1990 and 1991 (control group) and 258 chil-
1997 and living in the area between 1994 and 2002 were
dren born between 1992 and 1997 (study group)
analysed. Data for children born in the area were used
Born 1990 to 1991 Born 1992 to 1997
until the children had moved out of the area or died. Chil-
dren who had moved into the area were included in the fol-
low-up programme, but their results were analysed
The control group. There were 103 children born between
1990 and 1991; 87 lived in the area when the programme
started and 16 had moved in at a median age of nine years
(5 to 11; inter-quartile range 8 to 9). By January 1, 2003,
three children had died at six, nine and 11 years of age,
respectively. One child had moved out of the area at the age
The study group. There were 258 children born between
1992 and 1997; 210 were born in the area and 48 had
* GMFCS, gross motor function classification system
moved in at a median age of three years (0 to 9; inter-quar-tile range 2 to 5). Twenty-two children did not participatein the prevention programme. Four families declined to
1998 and 2002 in order to identify all children with prob-
participate, and 18 children were identified during the
able cerebral palsy.14 In those aged four years and older the
review undertaken in 2002 and then included in the pro-
diagnosis and subtypes of cerebral palsy were established.
gramme. However, information regarding their hips at the
The prevalence of children with cerebral palsy aged from
census date (January 1, 2003) was collected from their clin-
four to seven years and living in the area on January 1,
ical records. Of the remaining 236 children three had died
1998 was 2.4 per 1000 children.14 Our study of dislocation
at two, seven, and eight years of age, respectively, all from
of the hip also included children with cerebral palsy who
causes not related to the prevention programme. Four chil-
moved out of and into the area or died during the study
dren had moved out of the area at five, six, eight and nine
In addition to an active search for children with cerebral
The control and study groups were comparable with
palsy in order to offer them participation in the programme
regard to the proportion of subtype of cerebral palsy and
as early as possible, the health-care programme included a
GMFCS level (Table II). In the classification system,13 spas-
continuing standardised follow-up of the diagnosis, gross
tic diplegia includes all children in whom the lower limbs
motor function, clinical findings and treatment. The local
are more affected than the upper ones. This is in contrast to
physiotherapist and occupational therapist completed a
spastic tetraplegia which is defined as massive total motor
record twice a year until the age of six years and then once
disability with all four limbs severely involved, the upper
a year. The results were computerised and the local team
limbs at least as severely as the lower.
received a report showing the development of the child over
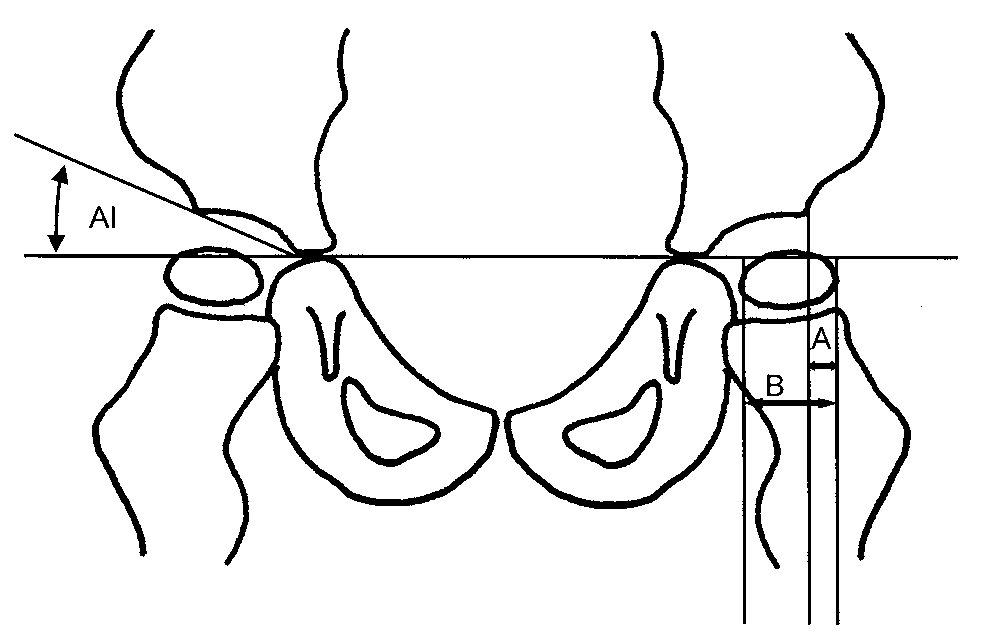
The migration percentage15 (MP) and acetabular index16
(AI) were measured on the radiographs (Fig. 1). All radio-
A standardised radiological follow-up of the hips was
graphs were assessed by one of the authors (GH). Both
carried out. They were examined on an anteroposterior
measurements have been shown to be reliable.15,17 How-
radiograph at diagnosis, then at least once a year in chil-
ever, recently some doubt on the inter- and intra-measurer
dren with the diplegic, tetraplegic or dystonic type cerebral
reliability has been raised, suggesting that repeated meas-
palsy until the age of eight years, and then on an individual
urements should be made by one individual.18 Hips with an
basis. Children with spastic hemiplegia or pure ataxia were
MP < 33% and an AI < 30˚ were regarded as normal. In
only examined radiologically at four years of age. The hip
children with lateral displacement or acetabular dysplasia,
programme began in 1994 and included children born in
the findings were compared with earlier measurements and
data from the physiotherapist’s follow-up. The decision
PREVENTION OF DISLOCATION OF THE HIP IN CHILDREN WITH CEREBRAL PALSY
osteotomy. Five children in the control group had beentreated by SDR, and three with ITB.
None of the 206 children monitored by the prevention
programme from the time of diagnosis has developed dislo-cation of the hip (p < 0.001). None of the 48 who movedinto the area between 1995 and 2002 developed any furtherdislocation.
One boy had a dislocated hip when he moved into the
area. One girl whose family were unwilling to participate inthe prevention programme has developed bilateral disloca-tion. One boy, born in 1993, with spastic tetraplegia had alateral displacement of the hips (MP 40 left, 74 right) at theage of three years. Operation by adductor-iliopsoas tenot-omy was recommended, but the child’s respiratory condi-
tion was such that he was only expected to survive for a
Diagram showing measurement of the acetabular index (AI) and migra-
short period. Surgery was therefore not undertaken. The
tion percentage (MP; MP = A/B x 100).
right hip dislocated within two years and the child died ateight years of age.
In the study group 50 children (78 hips) showed lateral-
with regard to preventative treatment was made together
isation of the hip with an MP exceeding 33% (Table III). At
with the child’s family and the local treatment team.
the date of census, 54 of these hips had been corrected to
In the younger and in older children with minor displace-
normal (MP < 33%). Of these, 11 were operated on by
ment, orthopaedic surgery usually involved bilateral tenot-
adductor-iliopsoas tenotomy, and 16 by proximal varus
omies of the adductors and iliopsoas. With marked
femoral osteotomy. Five children (six hips with lateralisa-
displacement, or if the lateral displacement was not reduced
tion) have been treated by SDR, and two children (three
within one year after adductor-iliopsoas tenotomy, a varus
hips) with ITB. In 18 hips the MP corrected to normal with
osteotomy of the proximal femur was performed. In chil-
no operative treatment. These hips had a mean MP of 35%
dren with marked dysplasia, acetabular reconstruction was
sometimes necessary. Post-operatively, the children were
At the date of census 24 hips still had an MP equal to or
treated by positioning the hips in extension and abduction
exceeding 33% (Table III). Three children (five lateralised
during lying and sitting. Standing frames and abduction
hips) had died. In nine hips the MP was decreasing, and in
splints were often used. Treatment with a hip spica plaster
two it remained at 33%. In seven hips preventative surgery
was planned. One child was operated on just before the
In children for whom reduction of spasticity was planned
using selective dorsal rhizotomy (SDR) or continuous infu-
The AI was increased (> 30˚) in 18 children (23 hips) in
sion of intrathecal baclofen (ITB), it was often possible to
the study group. The mean AI in these hips was 34˚ (30 to
wait and see if the decreased spasticity reduced lateral hip
40). All hips with an increased AI also had an MP greater
displacement. The indications for SDR and ITB were when
than 33%. At the census date the AI was normal in all
problems were directly related to increased muscle tone,
except seven hips. In one case, with an AI of 40˚, a pelvic
and the decision to employ such treatment was made irre-
osteotomy was performed after the date of census. It was
spective of the degree of lateralisation of the hip.
decreasing or approaching 30˚ in the remaining six hips. Statistical analysis. Fisher’s test was used to evaluate the
In total, 25 children, five in the control group and 20 in
efficiency of the prevention programme.
the study group, have been operated on by SDR at a medianof four years of age (3 to 6). Of these, 17 had normal hip
radiographs before and after operation. In the remaining
At the date of census, eight children in the control group
eight children, eight hips showed lateral migration before
had developed unilateral dislocation of the hip, always
SDR. In five hips the lateral migration corrected without
between the age of three and six years. All children with
further treatment post-operatively. In a further two hips the
dislocated hips had severe pain, at least periodically. All had
MP decreased, and in one hip it remained at 33%. Two hips
pelvic obliquity and scoliosis. In three patients, resection of
were normal before SDR, but have developed lateralisation
the femoral head and subtrochanteric valgus osteotomy
after the procedure. In one boy (case 24, Table III) the MP
were performed to reduce pain. Three of the children with
increased to 42% at eight years of age, and a varus femoral
dislocation had died. A further nine of the 103 children in
osteotomy was performed. In the other case the MP
the control group had developed lateral displacement. All
increased to 34%. This hip will be investigated by further
had been operated upon to prevent dislocation, six by
radiography before a decision is made regarding preventa-
adductor-iliopsoas tenotomy and three by varus femoral
G. HÄGGLUND, S. ANDERSSON, H. DÜPPE, H. LAUGE-PEDERSEN, E. NORDMARK, L. WESTBOM
Table III. Data on the 50 children (78 hips) with lateral migration in the study group Age at latest GMFCS† Highest operation follow-up MP at latest Diagnosis* MP (yrs) MP Treatment‡ follow-up Comments
Planned for new femoral + pelvic osteotomy
* according to Hagberg et al12; H, spastic hemiplegia; D, spastic diplegia; T, spastic triplegia; Dy, dystonic type; A, athetonic type† GMFCS, gross motor function classification system‡ 0, no treatment; ad, adductor-psoas tenotomy; ost, varus osteotomy of the proximal femur; SDR, selective dorsal rhizotomy; ITB, intrathecalbaclofen pump
PREVENTION OF DISLOCATION OF THE HIP IN CHILDREN WITH CEREBRAL PALSY
Table III (cont.) Data on the 50 children (78 hips) with lateral migration in the study group Age at latest GMFCS† Highest operation follow-up MP at latest Diagnosis* MP (yrs) MP Treatment‡ follow-up Comments
* according to Hagberg et al12; H, spastic hemiplegia; D, spastic diplegia; T, spastic triplegia; Dy, dystonic type; A, athetonic type† GMFCS, gross motor function classification system‡ 0, no treatment; ad, adductor-psoas tenotomy; ost, varus osteotomy of the proximal femur; SDR, selective dorsal rhizotomy; ITB, intrathecalbaclofen pump
Seven children have been treated with ITB, three in the
in southern Sweden, who have a dislocated hip. These are
control group and four in the study group. The hips in two
the boy who moved into the area with an established dislo-
children in the study group showed lateral displacement
cation and the girl who did not participate in the pro-
before treatment with ITB. At the date of census three of
these hips were normal and one showed an MP of 33%.
A dislocated hip in a child with cerebral palsy is a serious
problem. The reported frequency of children with pain var-
Discussion
ies, probably due to the difficulty in assessing pain in these
Of the 103 children in the control group, eight have devel-
children. Cooperman et al3 and Bagg et al5 who used stand-
oped dislocation of the hip. This cannot be looked upon as
ardised criteria for assessment of pain have reported the
the natural history of untreated hips. Some of the nine chil-
highest incidence of 50% to 90%. Pain often results in
dren operated upon for lateral displacement would proba-
increased muscle tone with increased energy requirements.
bly have had dislocation if they had not had the operation.
A child with dislocated hips often deteriorates with under-
Some of the children with lateral displacement and treated
nourishment, increased contractures, postural difficulties,
by SDR or with ITB could also have developed dislocation
skin ulceration and problems with perineal care. Perhaps it
of the hip. In the study group, 50 (21%) of 236 children
is no mere coincidence that four of the five children who
showed lateral displacement of the hip. The displacement
died at more than four years of age during the study period
returned to normal without operative treatment in 12. The
remaining 38 (16%) would probably have had dislocation
We chose an MP of 33% as the indication for interven-
without preventative surgery. This suggests that the natural
tion according to the definition of subluxation of Reim-
risk for hip dislocation in a total population of children
ers.15 Other reports have used an MP of 30% to 40% as the
with cerebral palsy is between 15% and 20%.
indication for surgery.20,21 Several hips with an MP
The children in the study group were aged between five
between 33% and 40% returned to normal levels without
and 11 years at the date of census. They are still at potential
operative treatment. These children had not received any
risk of dislocation, but they are older than the age at dislo-
additional non-operative treatment as a result of the radio-
cation in the control group, and it is known that most dis-
logical findings. No hip with an MP exceeding 42%
locations of the hip occur before seven years of age.19 The
returned to normal without operative treatment. We
lower incidence at this age in the study group as compared
recommend radiological follow-up at intervals of six
with the control group is statistically significant (p <
months before a decision about surgery is made in hips with
0.001). At present, there are only two children with cere-
an MP of between 33% and 40%, especially if the child is
bral palsy in a total of about 400 up to the age of 12 years
walking and has a good range of movement in the hip.
G. HÄGGLUND, S. ANDERSSON, H. DÜPPE, H. LAUGE-PEDERSEN, E. NORDMARK, L. WESTBOM
Radiographs showing the hips of a boy (case 32) with dystonic-type cerebral palsy, GMFCS 5. a) At five years of age witha migration percentage (MP) of 79% on the left and 33% on the right. He underwent bilateral adductor-psoas tenotomyand b) at ten years of age with an MP of 28% on the left and 58% on the right.
Radiographs showing the hips of a boy (case 13) with dystonic-type cerebral palsy, GMFCS 5. a) At three years of age with amigration percentage (MP) of 44% on the left and 50% on the right. He underwent bilateral adductor-psoas tenotomy, b) atfive years of age with an MP of 47% on the left and 73% on the right, c) after operation with proximal femoral varus osteotomyand d) at six years of age with an MP of 46 % on the left and 40% on the right.
PREVENTION OF DISLOCATION OF THE HIP IN CHILDREN WITH CEREBRAL PALSY
The AI was increased in 23 hips, all of which also
the hips, arranging radiological screening and the analysis
showed an increased MP. Our results do not support the
findings of Cooke, Cole and Carey22 that lateral displace-
In the future we hope to be able to discover which chil-
ment is always preceded by an increased AI. Our findings
dren in the population are at risk of dislocation of the hip in
indicate that the MP could be used as the only measurement
relation to subtype of cerebral palsy, function and other
in a screening programme for dislocation of the hip. It also
information from the collected data. We also hope to
suggests that lateral displacement precedes acetabular dys-
improve the timing of radiological examination and the
choice of intervention for lateral displacement.
Children with spastic hemiplegia and pure ataxia are
The study was supported by the Medical faculty, Lund University and Stiftelson
included in the radiological follow-up, but normally radio-
för bistånd åt vanföra i Skåne.
graphs were only taken at diagnosis and at four years of
No benefits in any form have been received or will be received from a com-
mercial party related directly or indirectly to the subject of this article.
age. One reason for their inclusion is that some childrenwith spastic diplegia in their early years may present withunilateral symptoms. Some children with ataxic diplegia
References
could present with mainly ataxic symptoms, and be initially
1. Howard CB, McKibbin B, Williams LA, Mackie I. Factors affecting the incidence
of hip dislocation in cerebral palsy. J Bone Joint Surg [Br] 1985;67-B:530-2. 2. Lonstein JE, Beck K. Hip dislocation and subluxation in cerebral palsy. J Pediatr
The combination of adduction and flexion spasticity or
contracture appears to cause the lateral displacement.23
3. Cooperman DR, Bartucci E, Dietrick E, Millar EA. Hip dislocation in cerebral
Soft-tissue surgery should address both of these deformi-
palsy: long-term consequences. J Pediatr Orthop 1987;7:268-76.
ties. We always combine adductor and iliopsoas tenotomy,
4. Moreau M, Drummond DS, Rogala EJ, Aschworth A, Porter T. Natural history of
dislocated hip in spastic cerebral palsy. Dev Med Child Neurol 1979;21:749-53.
and we always perform the surgery bilaterally in children
5. Bagg MR, Farber J, Miller F. Long-term follow-up of hip subluxation in cerebral
with bilateral spasticity or dystonia. If a child who cannot
palsy patients. J Pediatr Orthop 1993;13:32-6.
walk has a knee contracture exceeding 20˚, the knee is
6. Samilson RKL, Carson JJ, James P, Raney FL. Results and complications of
adductor tenotomy and obturator neurectomy in cerebral palsy. Clin Orthop
treated post-operatively by serial casting. The combination
of iliopsoas tenotomy and treatment of the knee contrac-
7. McIvor WC, Samilson RL. Fractures in patients with cerebral palsy. J Bone Joint
ture is probably the reason why no child has developed
8. Pritchett JW. The untreated unstable hip in severe cerebral palsy. Clin Orthop
hyperabduction post-operatively, a reported complica-
9. Letts M, Shapiro L, Mulder K, Klassen O. The windblown hip syndrome in total
Varus osteotomy of the proximal femur has been carried
body cerebral palsy. J Pediatr Orthop 1984;4:55-62.
out in 15 children (21 hips) in the study group. During the
10. Tachdjian MO, Minear WL. Hip dislocation in cerebral palsy. J Bone Joint Surg
first years of the programme some children were diagnosed
11. Mutch L, Alberman E, Hagberg B, Kodasma K, Perat MV. Cerebral palsy epide-
and referred late when it was considered to be too late for an
miology: where are we now and where are we going? Dev Med Child Neurol
adductor-psoas tenotomy. However, in doubtful cases, we
12. Hagberg B, Hagberg G, Olow I. The changing panorama of cerebral palsy in Swe-
often prefer to do an adductor-psoas tenotomy first. If no
den 1954-1970. Acta Paediatr Scand 1975;64:187-92.
decrease in lateral displacement is seen within one year, we
13. Palisano R, Rosenbaum P, Walter S, et al. Development and reliability of a sys-
perform a proximal varus femoral osteotomy (Figs 2 and 3).
tem to classify gross motor function in children with cerebral palsy. Dev Med ChildNeurol 1997;39:214-23.
The new techniques of reducing spasticity by SDR, ITB
14. Nordmark E, Hägglund G, Lagergren J. Cerebral palsy in southern Sweden: I prev-
and botulinum toxin have probably prevented lateral dis-
alence and clinical features. Acta Paediatr 2001;90:1271-6.
placement in some cases. In one boy a lateral displacement
15. Reimers J. The stability of the hip in children: a radiological study of the results of
of 44% corrected to normal within one year after treatment
muscle surgery in cerebral palsy. Acta Orthop Scand 1980;184(Suppl):1-97. 16. Hilgenreiner H. Zur frühdiagnose und frühbehandlung der angeborenen hüftgel-
with ITB. It has been suggested that SDR could increase the
lenkeverrenkung. Med Klin 1925;37-38:1385-429.
risk of dislocation by increasing the muscle imbalance at
17. Parrott JK, Boyd RN, Dip OG, et al. Hip displacement in spastic cerebral palsy: reli-
the hip.25 All children treated by SDR were operated upon
ability of radiological measures. J Paed Orthop 2002;22:660-7.
up to L2 and no signs of increased muscle imbalance were
18. Faraj S, Atherton WG, Stott NS. Inter- and intra-measurer error in the measure-
ment of Reimer’s hip migration percentage. J Bone Joint Surg [Br] 2004;86-B:434-7. 19. Rang M, Silver R, de la Garza J. Cerebral palsy. In: Lovell WW, Winter RB, eds.
The main challenge for this programme was the early
Pediatric orthopaedics. Second ed. Philadelphia: JB Lippincott Co, 1986:345-96.
identification of all children with cerebral palsy in the pop-
20. Onimus M, Allamel G, Manzone P, Laurain JM. Prevention of hip dislocation in
cerebral palsy by early psoas and adductors tenotomies. J Pediatric Surg
ulation.14 The health-care programme has been developed
in collaboration with the local child rehabilitation team of
21. Dobson F, Boyd RN, Parrott J, Nattrass GR, Graham HL. Hip surveillance in chil-
physiotherapists, occupational therapists, paediatricians
dren with cerebral palsy. J Bone Joint Surg [Br] 2002;84-B:720-6.
and orthopaedic surgeons. All interventions have the sup-
22. Cooke PH, Cole WG, Carey RPL. Dislocation of the hip in cerebral palsy. J Bone Joint Surg [Br] 1989;71-B:441-6.
port of both the local team and the paediatric orthopaedic
23. Kalen V, Bleck EE. Prevention of spastic paralytic dislocation of the hip. Dev Med
surgeon. This collaboration has been essential both to start
and run the programme. However, it is our experience that
24. Silver RL, Rang M, Chan J, de la Garza J. Adductor release in nonambulant chil-
dren with cerebral palsy. J Pediatr Orthop 1985;5:672-7.
once the child has been included in the follow-up pro-
25. Greene WB, Dietz FR, Goldberg MJ, et al. Rapid progression of hip subluxation in
gramme, an orthopaedic surgeon should be responsible for
cerebral palsy after selective posterior rhizotomy. J Pediatr Orthop 1991;11:494-7.
Interim Guidance on Antiviral Recommendations for Patients with Confirmed or Suspected Swine Influenza A (H1N1) Virus Infection and Close Contacts Objective: To provide interim guidance on the use of antiviral agents for treatment and chemoprophylaxis of swine influenza A (H1N1) virus infection. This includes patients with confirmed, probable or suspected swine influenza A (H1N1) virus
SAFETY DATA SHEET according to EC directive 1907/2006/EC 1. IDENTIFICATION OF THE SUBSTANCE/PREPARATION AND OF THE COMPANY/UNDERTAKING No particular dangers occur if the regulation/notes for storage and handling are observed. 2. COMPOSITION/INFORMATION ON INGREDIENTS NPK - fertilizer containing: Ammonium Nitrate, ammonium salts, phosphates, salts of calcium, potassium and possibly magnesi
 PREVENTION OF DISLOCATION OF THE HIP IN CHILDREN WITH CEREBRAL PALSY
osteotomy. Five children in the control group had beentreated by SDR, and three with ITB.
PREVENTION OF DISLOCATION OF THE HIP IN CHILDREN WITH CEREBRAL PALSY
osteotomy. Five children in the control group had beentreated by SDR, and three with ITB.




 G. HÄGGLUND, S. ANDERSSON, H. DÜPPE, H. LAUGE-PEDERSEN, E. NORDMARK, L. WESTBOM
Radiographs showing the hips of a boy (case 32) with dystonic-type cerebral palsy, GMFCS 5. a) At five years of age witha migration percentage (MP) of 79% on the left and 33% on the right. He underwent bilateral adductor-psoas tenotomyand b) at ten years of age with an MP of 28% on the left and 58% on the right.
G. HÄGGLUND, S. ANDERSSON, H. DÜPPE, H. LAUGE-PEDERSEN, E. NORDMARK, L. WESTBOM
Radiographs showing the hips of a boy (case 32) with dystonic-type cerebral palsy, GMFCS 5. a) At five years of age witha migration percentage (MP) of 79% on the left and 33% on the right. He underwent bilateral adductor-psoas tenotomyand b) at ten years of age with an MP of 28% on the left and 58% on the right.