Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Didattica.unibocconi.it
Adjuvant Chemotherapy Followed by Goserelin Versus Either Modality Alone for Premenopausal Lymph Node–Negative Breast Cancer: A Randomized Trial International Breast Cancer Study Group (IBCSG)1
Background: Although chemotherapy and ovarian function
Breast cancer is the most frequent non-cutaneous malignancy
suppression are both effective adjuvant therapies for pa-
diagnosed among women in the Western world (1). The majority
tients with early-stage breast cancer, little is known of the
of breast cancers are diagnosed at an operable stage, i.e., as a
efficacy of their sequential combination. In an International
primary tumor without or with axillary lymph node metastases
Breast Cancer Study Group (IBCSG) randomized clinical
but not widespread metastatic disease. Despite the considerable
trial (Trial VIII) for pre- and perimenopausal women with
number of putative prognostic factors that have been described
lymph node–negative breast cancer, we compared sequential
for breast cancer, the status of the axilla remains the most
chemotherapy followed by the gonadotropin-releasing hor-
important prognostic factor (2). Up to 80% of patients with
mone agonist goserelin with each modality alone. Methods:
newly diagnosed breast cancer in countries with mammographic
From March 1990 through October 1999, 1063 patients
screening programs do not have involvement of axillary lymph
stratified by estrogen receptor (ER) status and radiotherapy plan were randomly assigned to receive goserelin for 24
Despite undergoing radical surgery, some groups of patients
with lymph node–negative disease have recurrent disease at a
months (n ؍ 346), six courses of “classical” CMF (cyclophos-
rate exceeding 40% (3), possibly because of previously unde-
phamide, methotrexate, 5-fluorouracil) chemotherapy (n ؍
tected micro-metastases that later become overt. The aim of
360), or six courses of classical CMF followed by 18 months
systemic adjuvant therapy is the eradication or prevention of
of goserelin (CMF 3 goserelin; n ؍ 357). A fourth arm (no
disease progression or recurrence after surgery. Women receiv-
adjuvant treatment) with 46 patients was discontinued in
ing systemic adjuvant therapy have shown a clinically signifi-
1992. Tumors were classified as ER-negative (30%), ER-
cant improvement in both disease-free survival (DFS) and over-
positive (68%), or ER status unknown (3%). Twenty percent
all survival (OS) (4 – 6). Systemic adjuvant therapies include
of patients were aged 39 years or younger. The median
cytotoxic chemotherapy and endocrine therapies. Suppressed
follow-up was 7 years. The primary outcome was disease-
ovarian function, which reduces or eliminates estrogen produc-
free survival (DFS). Results: Patients with ER-negative tu-
tion, was the first adjuvant treatment studied in clinical trials
mors achieved better disease-free survival if they received CMF (5-year DFS for CMF ؍ 84%, 95% confidence interval [CI] ؍ 77% to 91%; 5-year DFS for CMF 3 goserelin ؍
1Writing Committee: Monica Castiglione-Gertsch, Anne O’Neill, Karen N. 88%, 95% CI ؍ 82% to 94%) than if they received goserelin
Price, Aron Goldhirsch, Alan S. Coates, Marco Colleoni, M. Laura Nasi, Marco
alone (5-year DFS ؍ 73%, 95% CI ؍ 64% to 81%). By contrast, for patients with ER-positive disease, chemother- Affiliations of Writing Committee members: International Breast Cancer Study
apy alone and goserelin alone provided similar outcomes
Group (IBCSG) Coordinating Center and Inselspital, Bern, Switzerland (MCG);
(5-year DFS for both treatment groups ؍ 81%, 95% CI ؍
IBCSG Statistical Center, Dana-Farber Cancer Institute, Harvard School of
76% to 87%), whereas sequential therapy (5-year DFS ؍
Public Health and Frontier Science and Technology Research Foundation, Bos-ton, MA (AO, KNP, MB, RDG); IBCSG Scientific Committee, European
86%, 95% CI ؍ 82% to 91%) provided a statistically non-
Institute of Oncology, Milan, Italy, and Oncology Institute of Southern Swit-
significant improvement compared with either modality
zerland, Bellinzona, Switzerland (AG); IBCSG Scientific Committee, University
alone, primarily because of the results among younger
of Sydney and The Cancer Council Australia, Sydney, Australia (ASC); European
women. Conclusions: Premenopausal women with ER-
Institute of Oncology, Milan (MC); IBCSG Coordinating Center, Bern (MLN). negative (i.e., endocrine nonresponsive), lymph node–nega- Correspondence to: Monica Castiglione-Gertsch, MD, IBCSG Coordi-
tive breast cancer should receive adjuvant chemotherapy.
nating Center, Effingerstrasse 40, CH-3008 Bern, Switzerland (e-mail: monica. castiglione@siak.ch). For patients with ER-positive (i.e., endocrine responsive) See “Appendix” for the names and affiliations of the participants and authors
disease, the combination of chemotherapy with ovarian func-
of the International Breast Cancer Study Group Trial VIII. tion suppression or other endocrine agents, and the use of See “Notes” following “References.”
endocrine therapy alone should be studied. [J Natl Cancer Inst 2003;95:1833– 46] Journal of the National Cancer Institute, Vol. 95, No. 24, Oxford UniversityPress 2003, all rights reserved.
Journal of the National Cancer Institute, Vol. 95, No. 24, December 17, 2003
involving premenopausal women. Suppressed ovarian function
with last normal menstrual period within 1 year, 2) aged 52 years
was achieved by surgical castration or by irradiation of the
or younger with last normal menstrual period within 3 years, 3)
ovaries. More recently, gonadotropin-releasing hormone agonist
aged 55 years or younger with hysterectomy but no bilateral
drugs such as goserelin have been used. Suppressed ovarian
oophorectomy (for patients aged older than 45 years, biochem-
function can also result from the use of cytotoxic agents. Patients
ical confirmation of ovarian function was requested), or 4)
who experienced amenorrhea, a consequence of suppressed
biochemical evidence of continuing ovarian function (for doubt-
ovarian function, after chemotherapy had longer disease-free
survival than patients who maintained ovarian function in some
All patients had a histologically proven unilateral breast
studies (7–11) but not in others (12–14). Thus, a controversy
cancer of stage T , T , T , T , T , N , or M [according to the
exists regarding the use of agents that suppress ovarian function
staging system of the Union Internationale Contre le Cancer
after chemotherapy (4). Five years of tamoxifen, the most com-
1987 (20)], with either ER-positive or ER-negative primary
mon endocrine therapy used in the adjuvant setting, has been
tumors. The ER-unknown status was allowed only if ER deter-
shown to be effective for reducing the risk of recurrent disease
mination was not possible because of the lack of tumor material.
and death in premenopausal and postmenopausal patients with
Steroid hormone receptor concentrations in the primary tumors
endocrine-responsive breast tumors (5).
were determined by standard methods (21,22). ER concentra-
In 1990, the International Breast Cancer Study Group
tions of at least 10 fmol/mg of cytosol protein by ligand-binding
(IBCSG) initiated a clinical trial (Trial VIII) for premenopausal
assay were considered positive; lower values were considered
and perimenopausal patients with lymph node–negative breast
negative. Determination of steroid hormone receptor status by
cancer to examine the role of adjuvant treatment using chemo-
immunohistochemistry was allowed later in the study. Conse-
therapy, ovarian suppression with goserelin, or the sequential
quently, ER status for 33% of the patients was determined by
combination of both modalities. Here, we provide the first report
immunohistochemistry, and participating center values for pos-
of results after a median follow-up of 7 years for women
Surgery to remove the primary tumor was either a total
mastectomy with axillary clearance or a conservative procedure
(quadrantectomy or lumpectomy) with axillary lymph node dis-
ATIENTS AND METHODS
section. Radiotherapy was recommended after breast-conserving
Study Design
surgery and was postponed until the end of chemotherapy, ifapplicable (23). Staging before randomization included chest
From March 1990 through October 1999, 1111 premeno-
x-ray, contralateral mammogram, bone scintogram (if clinically
pausal and perimenopausal patients were randomly assigned to
indicated), and hematologic, liver, and renal function tests.
receive no adjuvant systemic treatment, six 28-day courses of
Clinical, hematologic, and biochemical assessments were re-
“classical” CMF chemotherapy (in which one course consisted
quired every 3 months for the first year, every 6 months for the
of oral cyclophosphamide at 100 mg/m2 on days 1–14, intrave-
second year, and yearly thereafter. Modified World Health Or-
nous methotrexate at 40 mg/m2 on days 1 and 8, and intravenous
ganization toxicity grading criteria were used (24). Mammogra-
5-fluorouracil at 600 mg/m2 on days 1 and 8), 24 monthly
phy was performed yearly. The data management and medical
subcutaneous implants of goserelin (3.6 mg) every 28 days, or
staff reviewed all study records (initial data, treatment, toxicity,
six 28-day courses of classical CMF followed by 18 monthly
and recurrence) and conducted regular site visit audits. In par-
implants of goserelin. Systemic adjuvant therapy was to begin
ticular, the study chair (M. Castiglione-Gertsch) reviewed the
within 6 weeks of primary surgery. For the sequential treatment
records for all grade 3 or worse toxicities.
arm, the first goserelin implant was scheduled to be given on day28 of the sixth course of CMF. Informed consent was required
End Points and Statistical Considerations
according to the criteria established within the individual coun-tries. The protocol was reviewed and approved by institutional
Disease-free survival was defined as the length of time from
the date of randomization to any recurrent disease (including
In April 1992, on the basis of results from other trials (15–
ipsilateral breast recurrence), the appearance of a second pri-
18), randomization to the no-adjuvant-treatment control arm was
mary cancer (including contralateral breast cancer), or death,
discontinued. At that time, the trial had accrued 205 patients, 46
whichever occurred first. Overall survival was defined as the
of whom had been randomly assigned to the control arm. The
length of time from the date of randomization to death from any
results for this small initial cohort have been previously pub-
lished (19). This article reports the results of comparisons be-
Disease-free survival and overall survival percentages, stan-
tween the three active adjuvant-treatment arms.
dard errors, and treatment effect comparisons were obtained
Randomization was conducted centrally (at the coordinating
from the Kaplan–Meier method (25), Greenwood’s formula
centers in Bern, Switzerland, and Sydney, Australia) after strat-
(26), and log-rank tests (27), respectively. Cox proportional
ification according to estrogen receptor (ER) status (negative,
hazards regression models (28) were used to control for prog-
positive, or unknown), whether radiotherapy was planned after
nostic features, to estimate relative risks (RRs) and 95% confi-
breast-conserving surgery (yes or no), and by participating in-
dence intervals (CIs) for the treatment comparisons, and to test
stitution (see Appendix). The permuted blocks randomization
for interactions between potential predictive factors and treat-
schedule was produced by use of pseudorandom numbers gen-
ment effects. To check assumptions of proportionality, curves of
the log of the cumulative hazard for each value of a covariate
Pre- or perimenopausal status was defined as having one of
adjusted for other covariates in the model were plotted and
the following sets of characteristics: 1) aged older than 52 years
assessed visually to determine if the vertical shift between the
Journal of the National Cancer Institute, Vol. 95, No. 24, December 17, 2003
curves was constant over time. The data appeared to meet theassumptions of proportionality in all cases, with the exception ofage for the goserelin alone versus CMF alone comparison in theER-negative cohort. Adding an interaction term for age and timein the model for this treatment comparison did not change thetreatment effect estimate. All probability values were obtainedfrom two-sided tests. Results are reported at a median follow-upof 7 years.
Treatment– covariate interactions were studied by use of the
nonparametric Subpopulation Treatment Effect Pattern Plot(STEPP) methodology (29,30). STEPP involves defining severaloverlapping subgroups of patients on the basis of a covariate ofinterest and studying the resulting pattern of the treatment ef-fects estimated within each subgroup. In this article, patient age
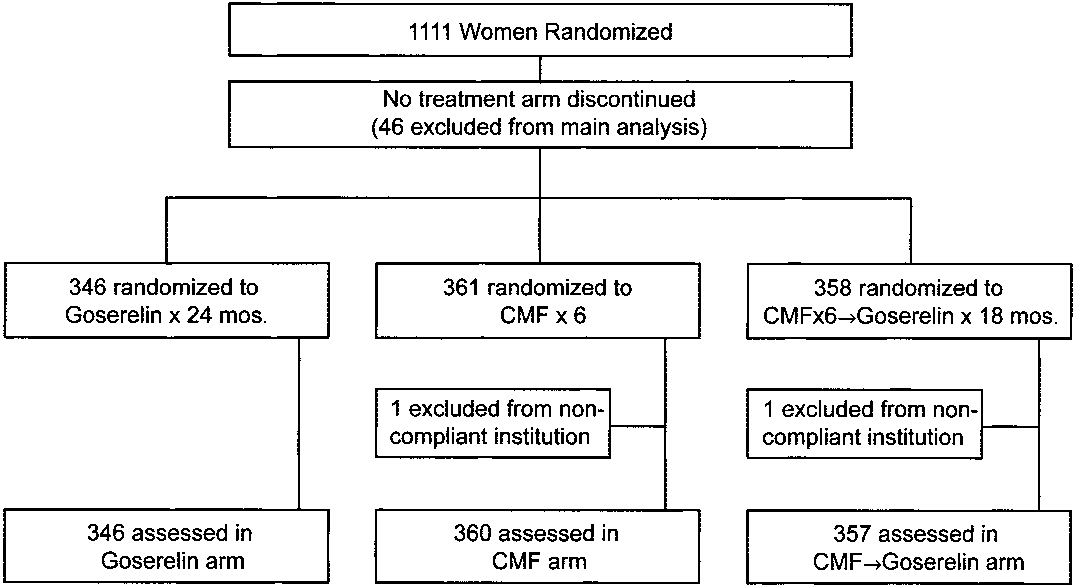
Fig. 1. Flow chart of enrollment and assessability for the primary analysis for
at study entry was the covariate of interest, and the treatment
patients enrolled in the International Breast Cancer Study Group (IBCSG) TrialVIII. CMF ϭ cyclophosphamide at 100 mg/m2 orally on days 1–14, methotrex-
effects estimated within each age subgroup were measured in
ate at 40 mg/m2 intravenously on days 1 and 8, and 5-fluorouracil at 600 mg/m2
terms of 5-year disease-free survival percentages, both overall
intravenously on days 1 and 8, repeated for six 28-day courses. mos. ϭ months.
and for cohorts defined according to ER status.
The intention to perform separate analyses according to ER
status was specified in the original protocol. After the closure of
the no-adjuvant-treatment control arm in 1992, the study was
Disease-Free Survival and Overall Survival
redesigned to assess whether six courses of CMF followed by 18implants of goserelin improved results relative to six courses of
Overall, no differences were observed among the three treat-
CMF alone (80% power to detect an improvement in 5-year DFS
ment groups (CMF chemotherapy, goserelin, CMF chemother-
from 80% to 88%) and whether 24 implants of goserelin and six
apy followed by goserelin) in terms of disease-free survival (Fig.
courses of CMF were comparable (95% chance to reject equiv-
2, A, and Table 2) or overall survival (Fig. 2, B). However,
alence if goserelin [72% 5-year DFS] was less effective than
differences among the treatment groups were suggested for
CMF [80% 5-year DFS]). Two hundred twenty-four events were
subpopulations defined according to ER status. Disease-free
required; 228 were observed at the time of this analysis.
survival for patients with ER-negative tumors who received
The Data and Safety Monitoring Committee reviewed accrual
CMF alone (5-year DFS ϭ 84%, 95% CI ϭ 77% to 91%) or
and safety data twice a year. Two predetermined interim efficacy
CMF followed by goserelin (5-year DFS ϭ 88%, 95% CI ϭ
analyses were performed (in December 1997 and June 2000),
82% to 94%) was greater than that for patients with ER-negative
and study continuation was recommended on both occasions. In
tumors who received only goserelin (5-year DFS ϭ 73%, 95%
1998, a protocol amendment restricted enrollment to patients
CI ϭ 64% to 81%) (Fig. 2, C, and Table 2). By contrast,
with ER-positive tumors on the basis of evidence from other
disease-free survival estimates for patients with ER-positive
trials that ovarian ablation might not be effective for patients
tumors who received CMF alone (5-year DFS ϭ 81%, 95% CI
ϭ 76% to 87%) or who received goserelin alone (5-year DFS ϭ81%, 95% CI ϭ 76% to 87%) were equivalent, whereas there
Patient Eligibility and Characteristics
was a modest, statistically nonsignificant advantage associatedwith the sequential administration of CMF followed by goserelin(5-year DFS ϭ 86%, 95% CI ϭ 82% to 91%) (Fig. 2, D, and
Of the 1111 patients randomly assigned, 46 were assigned to
Table 2). Unplanned, retrospective subgroup analyses according
the no-adjuvant-treatment arm and 1065 were assigned to one of
to age suggested that, among women with ER-negative tumors,
the three adjuvant-treatment arms (Fig. 1). Two patients enrolled
the superiority of the CMF-containing regimens compared with
from a noncompliant participating center were excluded from all
goserelin alone was seen for both older and younger women,
analyses. Of the remaining 1063 patients, 20 (1.9%) patients did
whereas for women with ER-positive tumors, the advantage of
not meet protocol eligibility criteria for the following reasons:
CMF followed by goserelin was seen only for younger women
postmenopausal status (n ϭ 11), in situ disease only (n ϭ 2),
resection margins involved with tumor (n ϭ 3), prior malig-
STEPP analyses were used to evaluate the differences in
nancy (n ϭ 2), lymph node–positive disease (n ϭ 1), and
treatment effects in terms of 5-year disease-free survival accord-
medical unsuitability (n ϭ 1). However, all 20 ineligible patients
ing to age (Fig. 3). For this sliding-window STEPP analysis,
are included in the intent-to-treat analyses.
each subpopulation contained approximately 165 patients, and
The characteristics of the 1063 assessable patients who were
each subsequent subpopulation was formed moving from left to
enrolled in active treatment arms are shown in Table 1. The
right by dropping approximately 30 patients with the lowest age
median age was 45 years (range ϭ 28 –58 years). Thirty percent
and adding approximately 30 patients with the next higher age.
(315) of the patients had primary tumors classified as ER-
The x coordinate indicates the median age for the patients in
negative (11% ER absent and 19% ER low), 68% (720) were
each subpopulation. The y coordinate indicates the 5-year
classified as ER-positive, and 3% (28) were classified as ER-
disease-free survival percent estimated using the Kaplan–Meier
unknown. The median number of axillary lymph nodes exam-
method on data from patients in each subpopulation. The results
ined was 16 (range ϭ 5– 60 lymph nodes).
for the entire study population show that, without separation of
Journal of the National Cancer Institute, Vol. 95, No. 24, December 17, 2003
Table 1. Patients’ characteristics according to treatment* All patients ER-negative cohort ER-positive cohort
*CMF ϫ 6 ϭ cyclophosphamide at 100 mg/m2 on days 1–14, orally; methotrexate at 40 mg/m2 on days 1 and 8, intravenously; and 5-fluorouracil at 600 mg/m2 on days 1 and 8,
intravenously; repeated for six 28-day courses. Goserelin ϫ 24 ϭ goserelin at 3.6 mg by subcutaneous implant monthly for 24 months. For the sequential combination therapy, CMF
ϫ 6 was followed by goserelin ϫ 18. 3 ϭ followed by; ER ϭ estrogen receptor; RT ϭ radiotherapy.
†ER status was determined by a ligand-binding assay for 67% of the patients and by immunohistochemistry for the other 33% of the patients (21,22). For the ligand-binding assay,
ER concentrations of at least 10 fmol/mg of cytosol protein were considered positive. For the immunohistochemistry, participating center values were used.
‡Tumor grade was determined at each participating site (31). §Methodologically, for tumors graded as grade 1, it is possible that the ER-negative classification might be false.
Journal of the National Cancer Institute, Vol. 95, No. 24, December 17, 2003
Fig. 2. Kaplan–Meier plots of disease-free survival (DFS) (panel A) and overall
or older in the ER-positive cohort (panel F). The number of patients, number of
survival (OS) (panel B) for 1063 pre- and perimenopausal women with lymph
DFS events, 5-year DFS % and 95% confidence interval (CI) for each treatment
node–negative breast cancer enrolled in the International Breast Cancer Study
group, and the relative risk of an event (recurrent disease, second malignancy, or
Group (IBCSG) Trial VIII according to randomized treatment group at a median
death), 95% CI, and P value for each pairwise treatment comparison for DFS are
follow-up of 7 years. Also shown are Kaplan–Meier plots of DFS for 315
shown in Table 2. For the overall survival in panel B, the 5-year OS % are 95%
patients in the estrogen receptor (ER)–negative cohort (panel C), for 720
(95% CI ϭ 93% to 97%; 35 deaths) for goserelin alone, 93% (95% CI ϭ 90%
patients in the ER-positive cohort (panel D), for 126 patients aged 39 years or
to 95%; 37 deaths) for CMF alone, and 95% (95% CI ϭ 93% to 97%; 27 deaths)
younger in the ER-positive cohort (panel E), and for 594 patients aged 40 years
Journal of the National Cancer Institute, Vol. 95, No. 24, December 17, 2003
Table 2. Disease-free survival (DFS) according to treatment*
*CMF ϫ 6 ϭ cyclophosphamide at 100 mg/m2 on days 1–14, orally; methotrexate at 40 mg/m2 on days 1 and 8, intravenously; and 5-fluorouracil at 600 mg/m2
on days 1 and 8, intravenously; repeated for six 28-day courses. Goserelin ϫ 24 ϭ goserelin at 3.6 mg by subcutaneous implant monthly for 24 months. For thesequential combination therapy, CMF ϫ 6 was followed by goserelin ϫ 18. CI ϭ confidence interval; ER ϭ estrogen receptor; 3 ϭ followed by.
†For each analysis, the relative risk is the risk of an event (recurrent disease, second malignancy, or death [Table 4]) for the first cohort listed compared with that
for the second cohort listed. A value greater than 1.00 indicates an increased risk of an event for the first cohort listed.
‡All statistical tests were two-sided.
the analysis according to ER status, there was no clear pattern of
status of the primary tumor, multiple regression analyses of
treatment differences according to age (Fig. 3, A). By contrast,
disease-free survival were conducted separately for the ER-
the CMF-containing regimens provide superior disease-free sur-
negative and ER-positive cohorts (Table 3). Factors for treat-
vival across all age groups for patients with ER-negative tumors
ment, age, primary therapy, tumor size, and tumor grade were
(Fig. 3, B), whereas the benefit of the sequential regimen for
included in all models. Treatment differences remained statisti-
patients with ER-positive disease increased substantially as the
cally significant for the ER-negative cohort, even after adjust-
median age of the patient subpopulation decreased below
ment for other factors. For the ER-positive cohort, age, primary
approximately age 43 years (Fig. 3, C). Fig. 3, C, also illustrates
treatment (increased risk of an event for breast-conserving sur-
that the equivalent outcome for CMF alone and goserelin alone
gery without radiotherapy), and tumor grade were prognostically
Interactions between the magnitude of treatment differences
and ER status were assessed using Cox proportional hazards
Incidence of Amenorrhea
models. Despite low statistical power, tests for interactions sug-gested that, compared with the CMF-containing regimens, gos-
The percentage of patients who reported no menses during
erelin alone was less effective for the ER-negative cohort than
each month after randomization according to treatment group is
for the ER-positive cohort (interactions: P ϭ .13 for goserelin
shown in Fig. 4. The percentage of patients who reported no
compared with the CMF– goserelin sequence and P ϭ .17 for
menses during each month from the no-adjuvant-therapy control
group is provided as an estimate for the natural rate of cessation
Considering the suggestive, statistically nonsignificant differ-
of menses associated with increasing age.
ences in treatment effect and the current approach of tailoring
For patients aged 39 years or younger (Fig. 4, A), goserelin
adjuvant therapy according to the steroid hormone receptor
induced amenorrhea within 2 months of study entry for 90% of
Journal of the National Cancer Institute, Vol. 95, No. 24, December 17, 2003
the end of six courses of CMF. Among patients in whomgoserelin was not given after CMF, menses resumed in approx-imately 15%, although amenorrhea continued in approximately35%– 40% of patients throughout the 36-month period of obser-vation. Among patients who received goserelin after CMF, vir-tually all achieved amenorrhea during the 18-month goserelintreatment period. Interestingly, resumption of menses after ces-sation of goserelin was slower in patients who had receivedinitial CMF chemotherapy than in those who did not receiveCMF chemotherapy, although menses did return in approxi-mately 40% of patients by the end of the 36-month follow-upperiod—the same percentage as among patients who had re-ceived goserelin alone.
The pattern of incidence of amenorrhea over time was dif-
ferent for patients aged 40 years or older at the time of studyentry (Fig. 4, B). The median age at study entry for this patientcohort was 46 years. Chemotherapy-induced amenorrhea wasobserved sooner and in a larger percentage of patients than wasobserved in the younger cohort. More than 90% of patients whoreceived six courses of CMF achieved amenorrhea by the end ofchemotherapy. Although menses resumed in a few patients whodid not receive goserelin after chemotherapy, a high incidence ofamenorrhea was observed during the entire 36-month follow-upperiod, regardless of whether goserelin was used. The incidenceof amenorrhea after completion of goserelin alone was the same(approximately 55%) as that observed for the no-adjuvant-therapy group during the third year of follow-up. Sites of Treatment Failure
Of the 1063 patients, 228 (21.4%) had recurrent disease or
died (Table 4). For the ER-negative cohort, the percentage ofpatients with visceral metastases was lower for the CMFgroup than for the goserelin alone group (difference ϭ 4.6%,95% CI ϭ Ϫ2.3% to 11.5%), and the percentage of patients withlocal recurrences was lower for the CMF followed by goserelingroup than for the goserelin alone group (difference ϭ 4.6%,95% CI ϭ Ϫ1.4% to 10.6%). For the ER-positive cohort, thepercentage of patients with local recurrences was lower for theCMF or CMF followed by goserelin groups than for the gosere-lin alone group (difference with CMF ϭ 4.3%, 95% CI ϭ 0.0%to 8.6%, and difference with CMF followed by goserelin ϭ3.0%, 95% CI ϭ Ϫ1.5% to 7.5%). Fig. 3. Subpopulation Treatment Effect Pattern Plots (STEPP) showing 5-year disease-free survival (DFS) percentage according to randomized treatment group CMF Treatment and Toxicity
and age for all patients (panel A), the estrogen receptor (ER)–negative cohort (panel B), and the ER-positive cohort (panel C) of women enrolled in the International Breast Cancer Study Group (IBCSG) Trial VIII. For this sliding-
Among the 717 patients randomly assigned to receive six
window STEPP analysis, each subpopulation contained approximately 165 pa-
courses of CMF (either alone or followed by goserelin), 646
tients, and each subsequent subpopulation was formed moving from left to right
(90%) completed all six courses, 55 (8%) received at least one
by dropping approximately 30 patients with the lowest age and adding approx-
but fewer than six courses, and 16 (2%) received no chemother-
imately 30 patients with the next higher age. The x coordinate indicates the
apy. Patient compliance was similar among treatment groups
median age for the patients in each subpopulation. The y coordinate indicates the5-year DFS percentage estimated using the Kaplan–Meier method on data from
regardless of whether CMF was followed by goserelin. Grade 3
or worse toxicities (primarily leukopenia, neutropenia, and nau-sea/vomiting) were experienced by 18.8% of the patients during
the patients and within 3 months for virtually all patients. Am-
CMF, including three life-threatening toxicities (two pulmonary
enorrhea continued until the end of treatment (i.e., at 24
embolisms and one cerebrovascular accident). There were no
months), when menses resumed in all but a few patients. By
treatment-related deaths. Of the 701 patients who received at
contrast, chemotherapy-induced amenorrhea was achieved more
least one course of CMF, 18.7% reported alopecia requiring
slowly and was observed in approximately 50% of patients by
Journal of the National Cancer Institute, Vol. 95, No. 24, December 17, 2003
Table 3. Multiple regression analyses of disease-free survival for estrogen receptor (ER)-negative and ER-positive cohorts*
Results of multiple regressions defined according to treatment comparison
ER-negative ER-positive
*CMF ϫ 6 ϭ cyclophosphamide at 100 mg/m2 on days 1–14, orally; methotrexate at 40 mg/m2 on days 1 and 8, intravenously; and 5-fluorouracil at 600 mg/m2
on days 1 and 8, intravenously; repeated for six 28-day courses. Goserelin ϫ 24 ϭ goserelin at 3.6 mg by subcutaneous implant monthly for 24 months. For thesequential combination therapy, CMF ϫ 6 was followed by goserelin ϫ 18. CI ϭ confidence interval; 3 ϭ followed by; Rx group ϭ treatment group indicatedat the top of the column; BCS ϭ breast-conserving surgery; RT ϭ radiotherapy.
†Relative risk for each analysis is the risk of an event (recurrent disease, second malignancy, or death [Table 4]) for the first cohort listed compared with that for
the second cohort listed. A value greater than 1.00 indicates an increased risk of an event for the first cohort listed.
‡All statistical tests (Wald test for single covariate; likelihood ratio test for multiple covariates) were two-sided. Models included indicator variables for unknown
§Methodologically, for tumors graded as grade 1, it is possible that the ER-negative classification might be false. Goserelin Treatment and Toxicity
patients assigned to the no-adjuvant-treatment group was lessthan that for patients in the three treatment groups combined, but
Among the 346 patients assigned to goserelin alone, 304
with the small number of patients, the difference was not statis-
(88%) received at least 22 implants, 36 (10%) received fewer
tically significant (P ϭ .19). Five-year disease-free survival
implants because of recurrent disease (5%) or other reasons
percentages (95% CI; sample size) were 61% (95% CI ϭ 47%
(5%), and six (2%) received no goserelin. Among the 357
to 75%; n ϭ 46) for no treatment, 73% (95% CI ϭ 62% to 84%;
patients assigned to goserelin following CMF, 289 (81%) re-
n ϭ 63) for goserelin alone, 79% (95% CI ϭ 67% to 91%; n ϭ
ceived at least 17 implants, 37 (10%) received fewer implants
43) for CMF alone, and 81% (95% CI ϭ 71% to 92%; n ϭ 53)
because of recurrent disease (3%) or other reasons (7%), and 31
for CMF followed by goserelin. The corresponding values for
(9%) received no goserelin. Grade 3 or worse toxicities (primar-
5-year disease-free survival percentages (95% CI; sample size)
ily weight gain) were experienced by 3.9% of the 666 patients
were 46% (95% CI ϭ 19% to 73%; n ϭ 13), 64% (95% CI ϭ
who received at least one goserelin implant (4.7% in the gos-
44% to 84%; n ϭ 22), 89% (95% CI ϭ 74% to 98%; n ϭ 18), 89%
erelin alone group and 3.1% in the goserelin following CMF
(95% CI ϭ 74% to 98%; n ϭ 18) for the ER-negative cohort and
group). One life-threatening (suicidal) depression was reported
67% (95% CI ϭ 50% to 84%; n ϭ 30), 73% (95% CI ϭ 58% to
during goserelin treatment (after 6 months of CMF and four
88%; n ϭ 34), 70% (95% CI ϭ 52% to 89%; n ϭ 24), 81% (95%
CI ϭ 68% to 95%; n ϭ 32) for the ER-positive cohort. Comparisons With No Adjuvant Treatment DISCUSSION
The median follow-up for the 205 patients who were enrolled
IBCSG Trial VIII for premenopausal and perimenopausal
before April 2, 1992, was 10.4 years. Disease-free survival for
women with lymph node–negative breast cancer began in 1990,
Journal of the National Cancer Institute, Vol. 95, No. 24, December 17, 2003
Ovarian function suppression was the first adjuvant systemic
treatment studied for patients with early-stage breast cancer(4,32–34). Chemotherapy is effective adjuvant therapy for pre-menopausal women (6). For several years, the effects of cyto-toxic agents on ovarian function were studied, but the interpre-tation of results remains controversial (7–14). The associationbetween chemotherapy-induced amenorrhea and outcome, how-ever, was confounded in retrospective analyses with chemother-apy dose intensity and duration. Although induction of amenor-rhea was found to be an important indicator of improvedoutcome for chemotherapy regimens that were less dose intenseand of shorter duration (7,8), the effect of amenorrhea on out-come was less evident when an intensive chemotherapy regimenwas used (12). Recently, however, a randomized trial showedstatistically significant increases in both the incidence of amen-orrhea and disease-free survival for very young patients (i.e.,aged 39 years or younger) with ER-positive tumors who re-ceived high-dose chemotherapy with peripheral blood progeni-tor cell support compared with standard doses of chemotherapy(35).
The incidence of amenorrhea was studied meticulously in
IBCSG Trial VIII. The spontaneous amenorrhea rate in our olderpatients (i.e., aged 40 years or older) was approximately 50% at3 years (Fig. 4, B, untreated group). We observed that the onsetof ovarian function suppression was delayed slightly for patientswho received chemotherapy relative to those who received go-serelin alone. However, despite this delay, the treatment out-come was similar for all three groups of older patients withendocrine-responsive disease (Fig. 2, F), whereas the combina-tion of the two modalities was better than the individual modal-ities for younger patients (i.e., those aged 39 years or younger)(Fig. 2, E). Although the underlying mechanism associated withthis observation is unclear, it is possible that if chemotherapycompletely suppressed ovarian function in the older patients,then subsequent treatment with goserelin may not have had theopportunity to improve outcome. This possibility might alsoexplain the observation in the Early Breast Cancer Trialists’Collaborative Group overview (4), which included mostlywomen aged 40 years or older and showed a lack of benefit ofoophorectomy when administered in addition to chemotherapy. Fig. 4. Percentage of patients enrolled in the International Breast Cancer Study
By contrast, for younger women in IBCSG Trial VIII, resump-
Group (IBCSG) Trial VIII with amenorrhea during each month from random-
tion of menses following completion of goserelin was slower
ization according to treatment. Panel A shows the results for patients aged 39
and occurred less often during the 36-month follow-up for
years or younger and panel B shows the results for patients aged 40 years or older.
women who received initial CMF chemotherapy than for thosewho received no CMF chemotherapy. Consequently, prolonged
when tamoxifen was not routinely used for premenopausal pa-
amenorrhea in a higher percentage of patients treated with
tients and when it was unclear whether ovarian function sup-
chemo-endocrine therapy than in those treated with endocrine
pression might be effective exclusively for patients with
therapy or chemotherapy alone may have contributed to the
endocrine-responsive disease (i.e., ER-positive tumors). Al-
prolonged disease-free survival associated with the combination
though overall the differences in disease-free survival among the
therapy observed in the younger cohort.
three treatment groups studied in IBCSG Trial VIII were not
Ovarian ablation (4), tamoxifen (5), and polychemotherapy
statistically significant, differential effects were observed when
(6) have all been shown to improve disease-free survival and
the analyses were conducted separately for the ER-negative and
overall survival, and their combined use has been the subject of
ER-positive cohorts. As expected today, for patients with ER-
continuing investigation. The combination of tamoxifen and
negative tumors, those who received CMF alone or followed by
ovarian function suppression was better than either treatment
goserelin had better disease-free survival than those who re-
individually for premenopausal patients with advanced breast
ceived goserelin alone. By contrast, for patients with ER-
cancer (36). The combination of tamoxifen plus goserelin was
positive tumors, the observed results for CMF alone and for
better than goserelin alone in the adjuvant setting following six
goserelin alone were equal, and the sequential use of CMF
courses of CAF (cyclophosphamide, adriamycin, fluorouracil)
followed by goserelin provided a statistically nonsignificant
chemotherapy (37). Among the several studies (38 – 41) that
benefit, primarily because of the results among younger women.
have compared adjuvant chemotherapy with endocrine therapies
Journal of the National Cancer Institute, Vol. 95, No. 24, December 17, 2003
Table 4. Sites of first treatment failure according to treatment*
% of total at a median follow-up of 7 years
*CMF ϭ six courses of cyclophosphamide at 100 mg/m2 on days 1–14, orally; methotrexate at 40 mg/m2 on days 1 and 8, intravenously; and 5-fluorouracil at
600 mg/m2 on days 1 and 8, intravenously. Goserelin ϭ goserelin at 3.6 mg by subcutaneous implant monthly for 24 months. For the sequential combination therapy,six courses of CMF was followed by 18 monthly implants of goserelin. ER ϭ estrogen receptor.
that consisted of 5 years of tamoxifen and 2 or 3 years of
with IBCSG Trial VIII, both trials were conducted almost ex-
gonadotropin-releasing hormone (Gn-RH) agonist, the largest
clusively in patients with lymph node–positive disease. The
has been the Austrian Breast and Colorectal Cancer Study Group
results of our study are similar to those of the Zoladex Early Breast
(ABCSG) Trial 5 (41), which yielded better results with com-
Cancer Research Association (ZEBRA) trial, which compared go-
bination endocrine treatment than with chemotherapy alone.
serelin for 2 years with CMF (intravenous, days 1 and 8, for six
Unfortunately, no trial has yet been conducted in the adjuvant
courses) in 1640 patients and had more than 7 years of follow-up
setting to compare tamoxifen plus ovarian function suppression
(45). The second trial (46), a multicenter study conducted in
with tamoxifen alone, either with or without chemotherapy.
France, compared adjuvant chemotherapy (anthracycline-based
However, this question is now being addressed by the global
for 77% of the patients) plus ovarian suppression (either ovarian
Suppression of Ovarian Function Trial (SOFT; coordinated by
irradiation or triptorelin for 3 years) with adjuvant chemotherapy
the IBCSG on behalf of the Breast International Group and the
alone in 926 patients. After 10 years of follow-up, the results
North American Breast Cancer Intergroup). SOFT compares
showed similar disease-free survival and overall survival for the
tamoxifen alone versus ovarian function suppression (by either
two treatment groups, which led the investigators to conclude
the Gn-RH analog triptorelin or bilateral oophorectomy or ovar-
that adjuvant chemotherapy and ovarian function suppression
ian irradiation) plus tamoxifen versus ovarian function suppres-
have a similar mechanism of antitumor activity (46). Because
sion plus exemestane (a steroidal aromatase inhibitor) for pa-
the mean age of the patients included in the French trial was 43
tients with steroid hormone receptor–positive tumors who
years and results were not provided for the youngest cohort, it is
remain premenopausal after adjuvant chemotherapy or for
not possible to assess the consistency of these findings with
whom tamoxifen alone is considered a reasonable treatment
option (42,43). The complementary Tamoxifen and Exemestane
IBCSG Trial IX found that CMF followed by tamoxifen was
Trial (TEXT) compares the Gn-RH analog triptorelin plus ta-
more effective than tamoxifen alone for postmenopausal patients
moxifen versus triptorelin plus exemestane for patients who
with lymph node–negative disease (47). In the present study, the
receive the Gn-RH analog with or without chemotherapy from
trial results confirm and extend the finding that chemotherapy is
the start of their adjuvant therapy program (42,43). Thus, the
more effective than endocrine therapy in terms of disease-free
roles of ovarian function suppression and of an aromatase in-
survival for patients with ER-negative tumors. The definition of
hibitor are being prospectively studied in the adjuvant setting for
ER-negative status on the basis of ligand-binding assay, how-
ever, represents a mixture of definitely endocrine-nonresponsive
tumors (i.e., an ER-absent cohort with no steroid hormone
IBCSG Trial VIII was designed at a time when the Early
receptor expression) and those with some modest responsiveness
Breast Cancer Trialists’ Collaborative Group overview analyses
to endocrine manipulations (i.e., an ER-low cohort with low
indicated that tamoxifen was not likely to be effective for
steroid hormone receptor expression). Thus, if the ER-absent
women younger than 50 years (44) and, thus, tamoxifen was not
cohort were to be considered separately, the differences in
included in the trial. Despite the absence of tamoxifen in the
outcome favoring the CMF-containing regimens compared with
study design, IBCSG Trial VIII is valuable for exploring the
goserelin alone may be greater than those observed. Further-
relationships among hormone receptor expression, short-
more, disease classified as ER-negative but progesterone recep-
duration ovarian function suppression, endocrine effects of che-
tor (PgR)-positive may also have some endocrine responsive-
motherapy, amenorrhea, and age. Two other trials (45,46) of
ness, because PgR status may be the dominant indicator for
adjuvant ovarian function suppression in premenopausal patients
endocrine responsiveness among premenopausal women (3). A
started accrual around the same time as IBCSG Trial VIII and
project is underway that will assess ER and PgR expression
also did not contain tamoxifen as a treatment option. By contrast
using quality-controlled immunohistochemical methodology in
Journal of the National Cancer Institute, Vol. 95, No. 24, December 17, 2003
a single laboratory for patients enrolled in IBCSG Trial VIII and
mone receptor–positive tumors who receive ovarian function
will assess outcomes separately for the ER- and PgR-absent and
suppression from the start of their adjuvant therapy program
ER- or PgR-positive cohorts (48). This investigation will also
clarify the relationship between steroid hormone receptor ex-
In addition to amenorrhea and ovarian function suppression,
pression, response to treatment, and the degree of overexpres-
cytotoxic chemotherapy may also have direct effects on
sion of c-erbB-2. The association with c-erbB-2 expression is
endocrine-responsive organs (52). Furthermore, the increased
important because the addition of ovarian ablation to tamoxifen
use of steroids as antiemetics and as supportive drugs for several
therapy has been shown to be effective, compared with no
old and new chemotherapy regimens (53) may provide addi-
adjuvant treatment, for patients with tumors overexpressing
tional antitumor effects for patients with endocrine-responsive
tumors. However, disease-free survival for women younger than
Very few of the premenopausal women enrolled in clinical
age 35 years with ER-positive tumors treated with either che-
trials that tested polychemotherapy (6) are young enough to
motherapy alone or with tamoxifen alone is statistically signif-
resist the effect of cytotoxic chemotherapy on ovarian endocrine
icantly worse than that for older premenopausal women (54 –
function, and thus allow the efficient testing of the role of further
56). Thus, it is important that alternative treatment approaches
ovarian suppression. In fact, we observed a most intriguing
such as ovarian function suppression with or without chemo-
finding in our subgroup of women younger than 40 years.
therapy be studied in young patients. In addition, serum endo-
Despite an earlier induction of ovarian function suppression with
crine level profiles and novel technologies should be developed
goserelin than with chemotherapy for this cohort of patients, it
to investigate endocrine effects of treatments in tumor stroma
was the women who received chemotherapy followed by gos-
and adjacent tissue, because resistance to endocrine therapies
erelin who had better disease-free survival. However, caution
and to the endocrine effects of chemotherapy may be related to
must be used when assessing the validity of results based on a
mechanisms that involve additional components of the tumor
retrospective subset analysis (50). Consequently, our observa-
microenvironment and not just to events in the tumor cells.
tion should not alter current patient care, but rather emphasizes
Endocrine therapies are important in the adjuvant treatment
the relevance of current studies of chemotherapy and endocrine
of young patients with endocrine-responsive early-stage breast
cancer. Because the diagnosis of breast cancer in young women
Premenopausal women with endocrine-responsive tumors,
is rare, widespread collaboration will be important to the suc-
especially those at low risk of recurrent disease, may not require
cessful conduct of relevant clinical trials such as the ongoing
chemotherapy provided they receive adequate endocrine ther-
Breast International Group/North American Breast Cancer In-
apy. To investigate this issue, the IBCSG conducted a random-
tergroup SOFT, TEXT, and PERCHE studies (42,43).
ized clinical trial in premenopausal women with lymph node–positive disease who received combined endocrine therapy with
APPENDIX
ovarian ablation (or suppression) and tamoxifen (51). In IBCSGTrial 11–93, four cycles of adjuvant chemotherapy (AC; doxo-
International Breast Cancer Study Group—Trial VIII partic-
rubicin at 60 mg/m2 or epirubicin at 90 mg/m2 plus cyclophos-
ipants and authors: Scientific Committee: A. Goldhirsch, A. S. Coates (co-chairs). Foundation Council: J. Collins (president), B.
phamide at 600 mg/m2, every 21 days) and ovarian function
Thu¨rlimann (vice president), H.-J. Senn (treasurer), S. Holmberg, J.
suppression (goserelin, bilateral oophorectomy, or ovarian irra-
Lindtner, A. Veronesi, H. Cortés-Funes. Coordinating Center,
diation) and 5 years of tamoxifen (20 mg/day) was compared
Bern, Switzerland: M. Castiglione-Gertsch (chief executive officer
with endocrine therapy (ovarian function suppression and ta-
and study chair), M. L. Nasi (studies coordinator), C. Jenatsch, G.
moxifen) alone. The study was small, with only 174 patients
Egli, M. Rabaglio, A. Saurer, R. Maibach, M. Iannino Gerber, A.
randomly assigned from May 1993 through November 1998.
Hiltbrunner. Statistical Center, Harvard School of Public Health
Ninety-five percent of the patients had one to three lymph nodes
and Dana-Farber Cancer Institute, Boston, MA: R. Gelber (group
involved, and 53% of the patients had only one lymph node
statistician), A. O’Neill, K. Price (scientific director), M. Bonetti, H.
involved. The median age was 45 years. After a median
Peterson, D. Zahrieh, M. Zelen, S. Gelber, A. Keshaviah, S. Li. Data
follow-up of 4.4 years, the 4-year disease-free survival Ϯ stan-
Management Center, Frontier Science and Technology Research Foundation, Amherst, NY: R. Hinkle, M. Isley, L. Blacher (direc-
dard error was 87% Ϯ 4% for the group that received AC and
tor), S. Lippert, J. Celano. Pathology Office: B. Gusterson, R.
88% Ϯ 4% for the endocrine therapy-alone group (RR for the
Bettelheim, R. Reed, G. Viale, E. Mallon. Quality of Life Office: J.
addition of AC ϭ 1.22, 95% CI ϭ 0.53 to 2.81; P ϭ .63),
Bernhard, C. Hu¨rny, H. Gusset, N. Mathys, B. Cliffe. The Ontario
suggesting that further study of the role of chemotherapy is
Cancer Treatment and Research Foundation, Toronto Sunny-
warranted in this setting. Today, virtually all premenopausal
brook Regional Cancer Centre, Toronto, Ontario, Canada: K.
women with lymph node–positive, steroid hormone receptor–
Pritchard, D. Sutherland, C. Sawka, G. Taylor, R. Choo, C.
positive disease receive chemotherapy, despite the absence of
Catzavelos, K. Roche. National Institute of Oncology, Budapest,
evidence showing that it is necessary for all such women. Hungary: I. La´ng, E. Hitre, E. Juhos, I. Szamel. Centro di Riferi-
Endocrine therapy alone with ovarian function suppression and
mento Oncologico, Aviano, Italy: D. Crivellari, S. Monfardini, E.
tamoxifen or an aromatase inhibitor may be sufficient to achieve
Galligioni, M. D. Magri, A. Veronesi, A. Buonadonna, S. Massarut,
excellent outcomes without chemotherapy, especially for pa-
C. Rossi, E. Candiani, A. Carbone, R. Volpe, M. Roncadin, M. Arcicasa, F. Coran, S. Morassut. Spedali Civili and Fondazione
tients at low risk of recurrent disease. This question is being
Beretta, Brescia, Italy: E. Simoncini, G. Marini, P. Marpicati, M.
investigated in the Premenopausal Endocrine Responsive Che-
Braga, P. Grigolato, L. Lucini. General Hospital, Gorizia, Italy: S.
motherapy (PERCHE) trial, which compares ovarian function
Foladore, L. Foghin, G. Pamich, C. Bianchi, B. Marino, A. Murgia,
suppression plus chemotherapy followed by tamoxifen or ex-
V. Milan. European Institute of Oncology, Milan, Italy: A. Gold-
emestane versus ovarian function suppression and tamoxifen or
hirsch, M. Colleoni, G. Martinelli, L. Orlando, F. Nolé, A. Luini, R.
exemestane without chemotherapy for patients with steroid hor-
Orecchia, G. Viale, F. Peccatori, F. de Braud, A. Costa, S. Zurrida,
Journal of the National Cancer Institute, Vol. 95, No. 24, December 17, 2003
P. Veronesi, V. Sacchini, V. Galimberti, M. Intra, U. Veronesi. Wales, Australia: M. Friedlander, B. Brigham, C. Lewis. Royal Ospedale Infermi, Rimini, Italy: A. Ravaioli, D. Tassinari, G. Adelaide Hospital, Adelaide, Australia: I. N. Olver, P. G. Gill, A.
Oliverio, F. Barbanti, P. Rinaldi, L. Gianni, G. Drudi. Ospedale S.
Taylor, D. Keefe. University of Sydney, Dubbo Base Hospital and Eugenio, Rome, Italy: M. Antimi, M. Minelli, V. Bellini, R. Porzio, Royal Prince Alfred Hospital, Sydney, Australia: J. Beith, M.
E. Pernazza, G. Santeusanio, L. G. Spagnoli. Ospedale S. Bortolo,
Boyer, A. S. Coates, R. J. Simes, A. Sullivan, M. H. N. Tattersall. Vicenza, Italy: M. Magazu, V. Fosser, P. Morandi, G. Scalco, M. W. P. Holman Clinic, Launceston, Australia: D. Boadle, I. Byard,
Balli, M. Gion, S. Meli, G. Torsello. The Institute of Oncology, Ljubljana, Slovenia: J. Lindtner, D. Erzen, E. Majdic, B. Stabuc, A. Plesnicar, R. Golouh, J. Lamovec, J. Jancar, I. Vrhoved, M. Kram- REFERENCES
berger. Groote Schuur Hospital and University of Cape Town, Cape Town, Republic of South Africa: D. M. Dent, A. Gudgeon, (1) Jemal A, Murray T, Samuels A, Ghafoor A, Ward E, Thun MJ. Cancer
E. Murray, I. D. Werner, P. Steynor, J. Toop, E. McEvoy. Sandton
statistics, 2003. CA Cancer J Clin 2003;53:5–26. Oncology Center, Johannesburg, Republic of South Africa: D. (2) Goldhirsch A, Glick JH, Gelber RD, Coates AS, Senn HJ. Meeting high-
Vorobiof, M. Chasen, G. Fotheringham, G. de Muelenaere, B. Sku-
lights: international consensus panel on the treatment of primary breast
dowitz, C. Mohammed, A. Rosengarten. Madrid Breast Cancer
cancer. Seventh International Conference on Adjuvant Therapy of Primary
Group, Madrid, Spain: H. Cortés-Funes, C. Mendiola, J. Hornedo,
Breast Cancer. J Clin Oncol 2001;19:3817–27.
R. Colomer, F. Cruz Vigo, P. Miranda, A. Sierra, F. Martinez-Tello,
(3) Colleoni M, Gelber S, Coates AS, Castiglione-Gertsch M, Gelber RD,
A. Garzon, S. Alonso, A. Ferrero. West Swedish Breast Cancer
Price K, et al., for the International Breast Cancer Study Group. Influence
Study Group, Göteborg, Sweden: C. M. Rudenstam, A. Wallgren,
of endocrine-related factors on response to perioperative chemotherapy for
S. Ottosson-Lönn, R. Hultborn, G. Colldahl-Ja¨derström, E. Cahlin,
patients with node-negative breast cancer. J Clin Oncol 2001;19:4141–9.
J. Mattsson, S. B. Holmberg, L. Ivarsson, O. Ruusvik, L. G. Niklas-
(4) Early Breast Cancer Trialists’ Collaborative Group. Ovarian ablation in
son, S. Dahlin, G. Karlsson, B. Lindberg, A. Sundba¨ck, S.
early breast cancer: overview of the randomised trials. Lancet 1996;348:
Bergegårdh, H. Salander, C. Andersson, M. Heideman, Y. Hessman,
O. Nelzén, G. Claes, T. Ramhult, J. H. Svensson, P. Liedberg, M. (5) Early Breast Cancer Trialists’ Collaborative Group. Tamoxifen for early
Suurku¨la, S. Persson. Swiss Group for Clinical Cancer Research
breast cancer: an overview of the randomised trials. Lancet 1998;351:1451– 67. (SAKK) member institutions—Inselspital, Bern, Switzerland: (6) Early Breast Cancer Trialists’ Collaborative Group. Polychemotherapy for
M. F. Fey, M. Castiglione-Gertsch, E. Dreher, H. Schneider, S. Aebi,
early breast cancer: an overview of the randomised trials. Lancet 1998;
J. Ludin, G. Beck, A. Haenel, J. M. Lu¨thi, H. J. Altermatt, M.
Nandedkar, K. Buser. Kantonsspital, St. Gallen, Switzerland: H. J. (7) Pagani O, O’Neill A, Castiglione-Gertsch M, Gelber RD, Goldhirsch A,
Senn, B. Thu¨rlimann, Ch. Oehlschlegel, G. Ries, M. Töpfer, U.
Rudenstam CM, et al. Prognostic impact of amenorrhoea after adjuvant
Lorenz, O. Schiltknecht, B. Spa¨ti, A. Ehrsam, M. Bamert, W. F.
chemotherapy in premenopausal breast cancer patients with axillary node
Jungi. Istituto Oncologico della Svizzera Italiana, Bellinzona,
involvement: results of the International Breast Cancer Study Group
Switzerland: F. Cavalli, O. Pagani, H. Neuenschwander, L. Bronz,
(IBCSG) trial VI. Eur J Cancer 1998;34:632– 40.
C. Sessa, M. Ghielmini, T. Rusca, P. Rey, J. Bernier, E. Pedrinis, T. (8) Goldhirsch A, Gelber RD, Castiglione M. The International Breast Cancer
Gyr, L. Leidi, G. Pastorelli, G. Caccia, A. Goldhirsch. Kantonsspi-
Study Group. The magnitude of endocrine effects of adjuvant chemother-
tal, Basel, Switzerland: R. Herrmann, C. F. Rochlitz, J. F. Harder,
apy for premenopausal breast cancer patients. Ann Oncol 1990;1:183– 8.
S. Bartens, U. Eppenberger, J. Torhorst. Hôpital des Cadolles, (9) Brincker H, Rose C, Rank F, Mouridsen HT, Jakobsen A, Dombernowsky
Neuchaˆtel, Switzerland: D. Piguet, P. Siegenthaler, V. Barrelet,
P, et al. Evidence of a castration-mediated effect of adjuvant cytotoxic
R. P. Baumann. University Hospital, Zu¨rich, Switzerland: B.
Pestalozzi, C. Sauter, D. Fink, M. Fehr, U. Haller, U. Metzger, P. (10) Padmanabhan N, Howell A, Rubens RD. Mechanism of action of adjuvant
Huguenin, R. Caduff. Centre Hospitalier Universitaire Vandois,
chemotherapy in early breast cancer. Lancet 1986;2:411– 4. Lausanne, Switzerland: L. Perey, S. Leyvraz, P. Anani, F. Gomez, (11) Minton SE, Munster PN. Chemotherapy-induced amenorrhea and fertility
D. Wellman, G. Chapuis, P. De Grandi, P. Reymond, M. Gillet, J. F.
in women undergoing adjuvant treatment for breast cancer. Cancer Control
Delaloye. Hôpital Cantonal, Geneva, Switzerland: P. Alberto, H.
Bonnefoi, P. Scha¨fer, F. Krauer, M. Forni, S. Diebold. Kantonsspi- (12) Parulekar W, Trudeau ME, Shepherd L, Ottaway J, Day A, Franssen E, et
tal Graubu¨nden, Chur, Switzerland: F. Egli, P. Forrer, A. Willi,
al. Incidence and prognostic impact of amenorrhea during adjuvant therapy
R. Steiner, J. Allemann, T. Ru¨edi, A. Leutenegger, U. Dalla Torre.
in high risk premenopausal breast cancer patients: analysis of a National
Australian New Zealand Breast Cancer Trials Group (ANZ
Cancer Institute of Canada Clinical Trials Group (NCIC CTG) phase III
BCTG) member institutions—Operations Office, University of
study [abstract 97]. Proc ASCO 2001;20:25A. Newcastle, Newcastle, Australia: J. F. Forbes, D. Lindsay, A. (13) Bonadonna G, Rossi A, Valagussa P, Banfi A, Veronesi U. The CMF
Wilson. Statistical Center, National Health and Medical Re-
program for operable breast cancer with positive axillary nodes: updated
search Council Clinical Trials Centre, University of Sydney,
analysis on the disease-free interval, site of relapse and drug tolerance. Camperdown, Australia: R. J. Simes, H. Dhillon. The Cancer Council Victoria (previously Anti-Cancer Council of Victoria), (14) Fisher B, Sherman B, Rockette H, Redmond C, Margolese R, Fisher ER. Clinical Trials Office, Melbourne, Australia: J. Collins, R. Sny-
1-Phenylalanine mustard (L-PAM) in the management of premenopausal
der, E. Abdi, A. Barling, R. Basser, W. I. Burns, M. Chipman,
patients with primary breast cancer: lack of association of disease-freesurvival with depression of ovarian function. National Surgical Adjuvant
J. Chirgwin, I. Davis, R. Holmes, M. Green, D. Hastrich, P. Gregory,
Project for Breast and Bowel Cancers. Cancer 1979;44:847–57.
R. McLennan, L. Mileshkin, P. Mitchell, G. Richardson, M. (15) Fisher B, Costantino J, Redmond E, Poisson R, Bowman D, Couture J, et
Schwarz, I. Russell, C. Underhill, D. Reading, A. Zimet. Auckland
al. A randomized clinical trial evaluating tamoxifen in the treatment of
Breast Cancer Study Group, Auckland, New Zealand: V. J.
patients with node-negative breast cancer who have estrogen-receptor
Harvey, P. Thompson, D. Porter. Flinders Medical Centre, Bed-
positive tumors. N Engl J Med 1989;320:479 – 84. ford Park, South Australia: T. Malden. Newcastle Mater Miseri- (16) Fisher B, Redmond C, Dimitrov NV, Bowman D, Legault-Poisson S,
cordiae Hospital Waratah, Newcastle, Australia: J. F. Forbes, J.
Wickerham DL, et al. A randomized clinical trial evaluating sequential
Stewart, D. Jackson, R. Gourlay, J. Bishop, S. Cox, S. Ackland, A.
methotrexate and fluorouracil in the treatment of patients with node-
Bonaventura, C. Hamilton, J. Denham, P. O’Brien, M. Back, S.
negative breast cancer who have estrogen-receptor-negative tumors.
Brae, R. Muragasu. Prince of Wales, Randwick, New South
Journal of the National Cancer Institute, Vol. 95, No. 24, December 17, 2003
(17) Mansour EG, Gray R, Shatila AH, Osborne CK, Tormey DC, Gilchrist
(37) Davidson N, O’Neill A, Vukov A, Osborne CK, Martino S, White D, et al.
KW, et al. Efficacy of adjuvant chemotherapy in high-risk node-negative
Effect of chemohormonal therapy in premenopausal node (ϩ) receptor (ϩ)
breast cancer. An intergroup study. N Engl J Med 1989;320:485–90.
breast cancer: an Eastern Cooperative Oncology Group phase III intergroup
(18) Ludwig Breast Cancer Study Group. Prolonged disease-free survival after
trial (E5188, INT-0101) [abstract 249]. Proc ASCO 1999;18:67a.
one course of perioperative adjuvant chemotherapy for node-negative
(38) Roché H, Mihura J, de Lafontan B, Reme-Saumon M, Martel P, Dubois J,
breast cancer. N Engl J Med 1989;320:491– 6.
et al. Castration and tamoxifen versus chemotherapy (FAC) for premeno-
(19) Castiglione-Gertsch M, Gelber RD, O’Neill A, Coates AS, Goldhirsch A. The
pausal, node and receptors positive breast cancer patients: a randomized
International Breast Cancer Study Group. Systemic adjuvant treatment for
trial with a 7 years median follow up [abstract 134]. Proc ASCO 1996;15:117.
premenopausal node-negative breast cancer. Eur J Cancer 2000;36:549 –50. (39) Roché HH, Kerbrat P, Bonneterre J, Fargeot P, Fumoleau P, Monnier A, et
(20) Hermanek P, Sobin LH, editors. TNM classification of malignant tumors.
al. Complete hormonal blockade versus chemotherapy in premenopausal
4th ed. Berlin (Germany): Springer-Verlag; 1987.
early-stage breast cancer patients (pts) with positive hormone-receptor
(21) Davis BW, Zava DT, Locher GW, Goldhirsch A, Hartmann WH. Receptor
(HRϩ) and 1–3 node-positive (Nϩ) tumors: results of the FASG 06 trial
heterogeneity of human breast cancer as measured by multiple intratumoral
[abstract 279]. Proc ASCO 2000;19:72a.
assays of estrogen and progesterone receptor. Eur J Cancer Clin Oncol
(40) Boccardo F, Rubagotti A, Amoroso D, Mesiti M, Romeo D, Sismondi P, et
al. Cyclophosphamide, methotrexate, and fluorouracil versus tamoxifen
(22) Berger U, Wilson P, McClelland RA, Davidson J, Coombes RC. Correla-
plus ovarian suppression as adjuvant treatment of estrogen receptor-
tion of immunocytochemically demonstrated estrogen receptor distribution
positive pre-/perimenopausal breast cancer patients: results of the Italian
and histopathologic features in primary breast cancer. Hum Pathol 1987;
Breast Cancer Adjuvant Study Group 02 randomized trial. J Clin Oncol
(23) Wallgren A, Bernier J, Gelber RD, Goldhirsch A, Roncadin M, Joseph D,
(41) Jakesz R, Hausmaninger H, Kubista E, Gnant M, Menzel C, Bauernhofer
et al., for the International Breast Cancer Study Group. Timing of radio-
T, et al. Randomized adjuvant trial of tamoxifen and goserelin versus
therapy and chemotherapy following breast-conserving surgery for patients
cyclophosphamide, methotrexate, and fluorouracil: evidence for the supe-
with node-positive breast cancer. Int J Radiat Oncol Biol Phys 1996;35:
riority of treatment with endocrine blockade in premenopausal patients
with hormone-responsive breast cancer–Austrian Breast and Colorectal
(24) Crivellari D, Bonetti M, Castiglione-Gertsch M, Gelber RD, Rudenstam
Cancer Study Group Trial 5. J Clin Oncol 2002;20:4621–7.
CM, Thu¨rlimann B, et al., for the International Breast Cancer Study Group. (42) Gelber RD, Castiglione-Gertsch M, Coates AS, Goldhirsch A, for the
Burdens and benefits of adjuvant cyclophosphamide, methotrexate, and
International Breast Cancer Study Group (IBCSG); Breast International
fluorouracil and tamoxifen for elderly patients with breast cancer: the
Group (BIG); North American Breast Intergroup. Tailored treatment in-
International Breast Cancer Study Group Trial VII. J Clin Oncol 2000;18:
vestigations for premenopausal women with endocrine responsive (ERϩ
and/or PgRϩ) breast cancer: the open questions [abstract P103]. The Breast
(25) Kaplan EL, Meier P. Nonparametric estimation from incomplete observa-
tions. J Am Stat Assoc 1958;53:457– 81. (43) Francis P, Fleming G, Nasi ML, Pagani O, Perez E, Walley B, for the
(26) Greenwood M. The natural duration of cancer. London (U.K.): Her Maj-
International Breast Cancer Study Group (IBCSG); Breast International
esty’s Stationary Office; 1926. p. 1–26.
Group (BIG); North American Breast Intergroup. Tailored treatment in-
(27) Mantel N. Evaluation of survival data and two new rank order statistics
vestigations for premenopausal women with endocrine responsive (ERϩ
arising in its consideration. Cancer Chemother Rep 1966;50:163–70.
and/or PgRϩ) breast cancer: the SOFT, TEXT, and PERCHE Trials
(28) Cox DR. Regression models and life-tables (with discussion). J Royal Stat
[abstract P104]. The Breast 2003;12 (Suppl 1):S44. (44) Early Breast Cancer Trialists’ Collaborative Group. Systemic treatment of
(29) Bonetti M, Gelber RD. A graphical method to assess treatment-covariate
early breast cancer by hormonal, cytotoxic, or immune therapy. 133 ran-
interactions using the Cox model on subsets of the data. Stat Med 2000;
domised trials involving 31,000 recurrence and 24,000 deaths among
75,000 women. Lancet 1992;339:1–15, 71– 85. (30) Bonetti M, Gelber RD, Goldhirsch A, Castiglione-Gertsch M, Coates AS,
(45) Kaufmann M, Jonat W, Blamey R, Cuzick J, Namer M, Fogelman I, et al.
for The International Breast Cancer Study Group (IBCSG). Features that
Survival analyses from the ZEBRA study: goserelin (Zoladex) versus CMF
predict responsiveness to chemotherapy and endocrine therapies. The
in premenopausal women with node-positive breast cancer. Eur J Cancer
(31) Davis BW, Gelber RD, Goldhirsch A, Hartmann WH, Locher GW, Reed R,
et al. Prognostic significance of tumor grade in clinical trials of adjuvant
(46) Arriagada R, Le MG, Spielmann M, Mauriac L, Bonneterre J, Namer M, et
therapy for breast cancer with axillary lymph node metastasis. Cancer
al. Randomized trial of adjuvant ovarian suppression in 926 premenopausal
patients with early breast cancer treated with adjuvant chemotherapy [ab-
(32) Meakin JW, Hayward JL, Panzarella T, Allt WE, Beale FA, Bulbrook RD,
et al. Ovarian irradiation and prednisone following surgery and radiother-
(47) International Breast Cancer Study Group. Endocrine responsiveness and
apy for carcinoma of the breast. Breast Cancer Res Treat 1996;37:11–9.
tailoring adjuvant therapy for postmenopausal lymph node-negative breast
(33) Cole MP. Prophylactic compared with therapeutic x-ray artificial meno-
cancer: a randomized trial. J Natl Cancer Inst 2002;94:1054 – 65.
pause. In: Joslin CA, Gleave EN, editors. The clinical management of
(48) Goldhirsch A, Wood WC, Gelber RD, Coates AS, Thu¨rlimann B, Senn HJ.
advanced breast cancer. 2nd Tenovus workshop. Cardiff, Wales (U.K.):
Meeting highlights: updated international expert consensus on the primary
Alpha Omega Alpha Publishing; 1970. p. 2–11.
therapy of early breast cancer. J Clin Oncol 2003;21:3357– 65. (34) Ravdin RG, Lewison EF, Slack NH, Dao TL, Gardner B, State D, et al. (49) Love RR, Duc NB, Havighurst TC, Mohsin SK, Zhang Q, DeMets DL, et
Results of a clinical trial concerning the worth of prophylactic oophorec-
al. HER-2/neu overexpression and response to oophorectomy plus tamox-
tomy for breast carcinoma. Surg Gynecol Obstet 1970;131:1055– 64.
ifen adjuvant therapy in estrogen receptor-positive premenopausal women
(35) Basser R, O’Neill A, Martinelli G, Nasi ML, Peccatori F, Cinieri S, et al.
with operable breast cancer. J Clin Oncol 2003;21:453–7.
Randomized trial comparing up-front, multi-cycle, dose-intensive chemo-
(50) Coates AS, Goldhirsch A, Gelber RD. Overhauling the breast cancer
therapy (CT) versus standard dose CT in women with high-risk stage 2 or
overview: are subsets subversive? Lancet Oncol 2002;3:525– 6.
3 breast cancer (BC): first results from IBCSG Trial 15–95 [abstract 20]. (51) International Breast Cancer Study Group. Randomized controlled trial of
ovarian function suppression plus tamoxifen versus the same endocrine
(36) Klijn JG, Blamey RW, Boccardo F, Tominaga T, Duchateau L, Sylvester
therapy plus chemotherapy: is chemotherapy necessary for premenopausal
R, et al., for the Combined Hormone Agents Trialists Group and the
women with node-positive, endocrine responsive breast cancer? First re-
European Organization for Research and Treatment of Cancer. Combined
sults of International Breast Cancer Study Group Trial 11–93. The Breast
tamoxifen and luteinizing hormone-releasing hormone (LHRH) agonist
versus LHRH agonist alone in premenopausal advanced breast cancer: a
(52) Morgan MW, O’Hare MJ. Cytotoxic drugs and the human adrenal cortex:
meta-analysis of four randomized trials. J Clin Oncol 2001;19:343–53.
a cell culture study. Cancer 1979;43:969 –79.
Journal of the National Cancer Institute, Vol. 95, No. 24, December 17, 2003
(53) Nabholtz JM, Pienkowski T, Mackey J, Pawlicki M, Guastalla JP, Vogel C,
tion, data management, and statistics was provided for the International
et al. Phase III trial comparing TAC (docetaxel, doxorubicin, cyclophos-
Breast Cancer Study Group by the Swedish Cancer Society, The Cancer
phamide) with FAC (5-fluorouracil, doxorubicin, cyclophosphamide) in the
Council Australia, the Australian New Zealand Breast Cancer Trials Group
adjuvant treatment of node positive breast cancer (BC) patients: interim
(NHMRC grants 890028, 920876, 950328, 980379, 141711), the Frontier
analysis of the BCIRG 001 study [abstract 141]. Proc ASCO 2002;21:36A.
Science and Technology Research Foundation, the Swiss Group for Clinical
(54) Aebi S, Gelber S, Castiglione-Gertsch M, Gelber RD, Collins J, Thu¨rli-
Cancer Research (SAKK), the Swiss Cancer League, the American–Italian
mann B, et al., for the International Breast Cancer Study Group. Is che-
Cancer Foundation (AICF grants 101-98 and 101-99), the American Cancer
motherapy alone adequate for young women with oestrogen-receptor-
Society (grant RPG-90-013-08-PBP), and Public Health Service grant CA-
positive breast cancer? Lancet 2000;355:1869 –74.
75362 from the National Cancer Institute, National Institutes of Health,
(55) Goldhirsch A, Gelber RD, Yothers G, Gray RJ, Green S, Bryant J, et al.
Department of Health and Human Services. We also acknowledge support for
Adjuvant therapy for very young women with breast cancer: need for
the Cape Town participants from the Cancer Association of South Africa, for
tailored treatments. J Natl Cancer Inst Monogr 2001;(30):44 –51.
the St. Gallen participants from the Foundation for Clinical Research of
(56) Aebi S, Castiglione-Gertsch M. Adjuvant endocrine therapy for the very
Eastern Switzerland, and for the Göteborg participants from the Swedish
young patients. Corrected proof. The Breast (DOI:10.1016/S0960-9776
Society for Cancer Research (Cancerfonden). Astra-Zeneca provided the
We thank the patients, physicians, nurses, and data managers who participate
in the International Breast Cancer Study Group trials. We thank Rita Hinkle fordata management.
Initial support was provided by the Ludwig Institute for Cancer Research
Manuscript received June 24, 2003; revised October 1, 2003; accepted
and the Cancer League of Ticino. Continuing support for central coordina-
Vascular II 0247 The Consequences of Socio-Economic status on outcomes from Amputation R. Gohil*, R. Barnes, I.C. Chetter Hull York Medical School, University of Hull, Hull & E Yorkshire Hospitals Trust, Hull, UK Aims : Currently 5,000 leg amputations occur annually in England and Wales and have a 50% mortality rate at 2 years. We aimed to analyse the effect of socioeconomic de
RODNEY’S RAVINGS take an open-minded and at times irreverent look at topical economic issues. Unlike our pay-to-view reports that are for the eyes of subscribers only, the RAVINGS are free and you may forward them to other p eople. You can signup to the RAVINGS on our website – http://www.sra.co.nz/lists/. The sa me distribution listed is used for the Property Insights repo
 curves was constant over time. The data appeared to meet theassumptions of proportionality in all cases, with the exception ofage for the goserelin alone versus CMF alone comparison in theER-negative cohort. Adding an interaction term for age and timein the model for this treatment comparison did not change thetreatment effect estimate. All probability values were obtainedfrom two-sided tests. Results are reported at a median follow-upof 7 years.
curves was constant over time. The data appeared to meet theassumptions of proportionality in all cases, with the exception ofage for the goserelin alone versus CMF alone comparison in theER-negative cohort. Adding an interaction term for age and timein the model for this treatment comparison did not change thetreatment effect estimate. All probability values were obtainedfrom two-sided tests. Results are reported at a median follow-upof 7 years.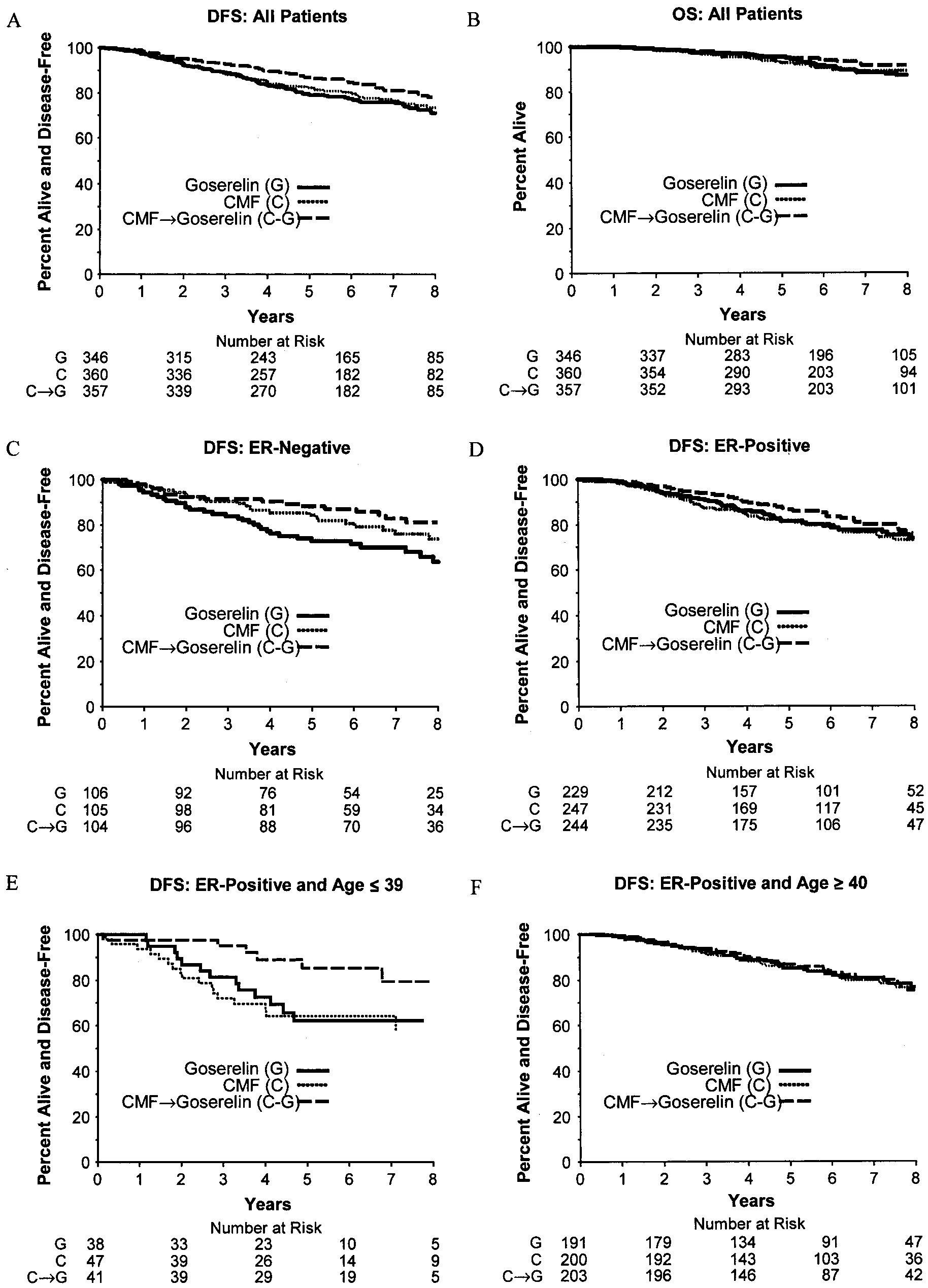 Fig. 2. Kaplan–Meier plots of disease-free survival (DFS) (panel A) and overall
Fig. 2. Kaplan–Meier plots of disease-free survival (DFS) (panel A) and overall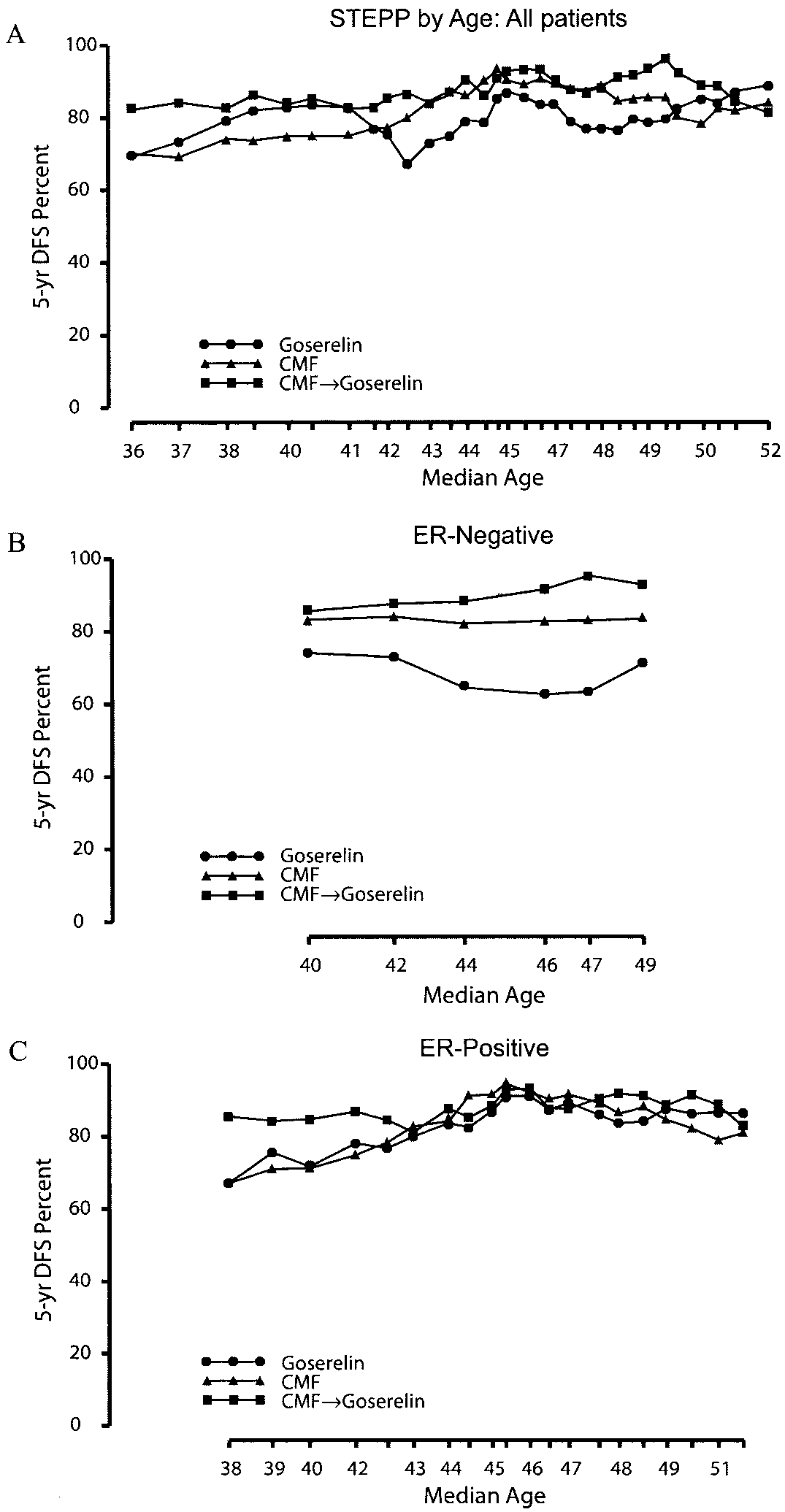 the end of six courses of CMF. Among patients in whomgoserelin was not given after CMF, menses resumed in approx-imately 15%, although amenorrhea continued in approximately35%– 40% of patients throughout the 36-month period of obser-vation. Among patients who received goserelin after CMF, vir-tually all achieved amenorrhea during the 18-month goserelintreatment period. Interestingly, resumption of menses after ces-sation of goserelin was slower in patients who had receivedinitial CMF chemotherapy than in those who did not receiveCMF chemotherapy, although menses did return in approxi-mately 40% of patients by the end of the 36-month follow-upperiod—the same percentage as among patients who had re-ceived goserelin alone.
the end of six courses of CMF. Among patients in whomgoserelin was not given after CMF, menses resumed in approx-imately 15%, although amenorrhea continued in approximately35%– 40% of patients throughout the 36-month period of obser-vation. Among patients who received goserelin after CMF, vir-tually all achieved amenorrhea during the 18-month goserelintreatment period. Interestingly, resumption of menses after ces-sation of goserelin was slower in patients who had receivedinitial CMF chemotherapy than in those who did not receiveCMF chemotherapy, although menses did return in approxi-mately 40% of patients by the end of the 36-month follow-upperiod—the same percentage as among patients who had re-ceived goserelin alone.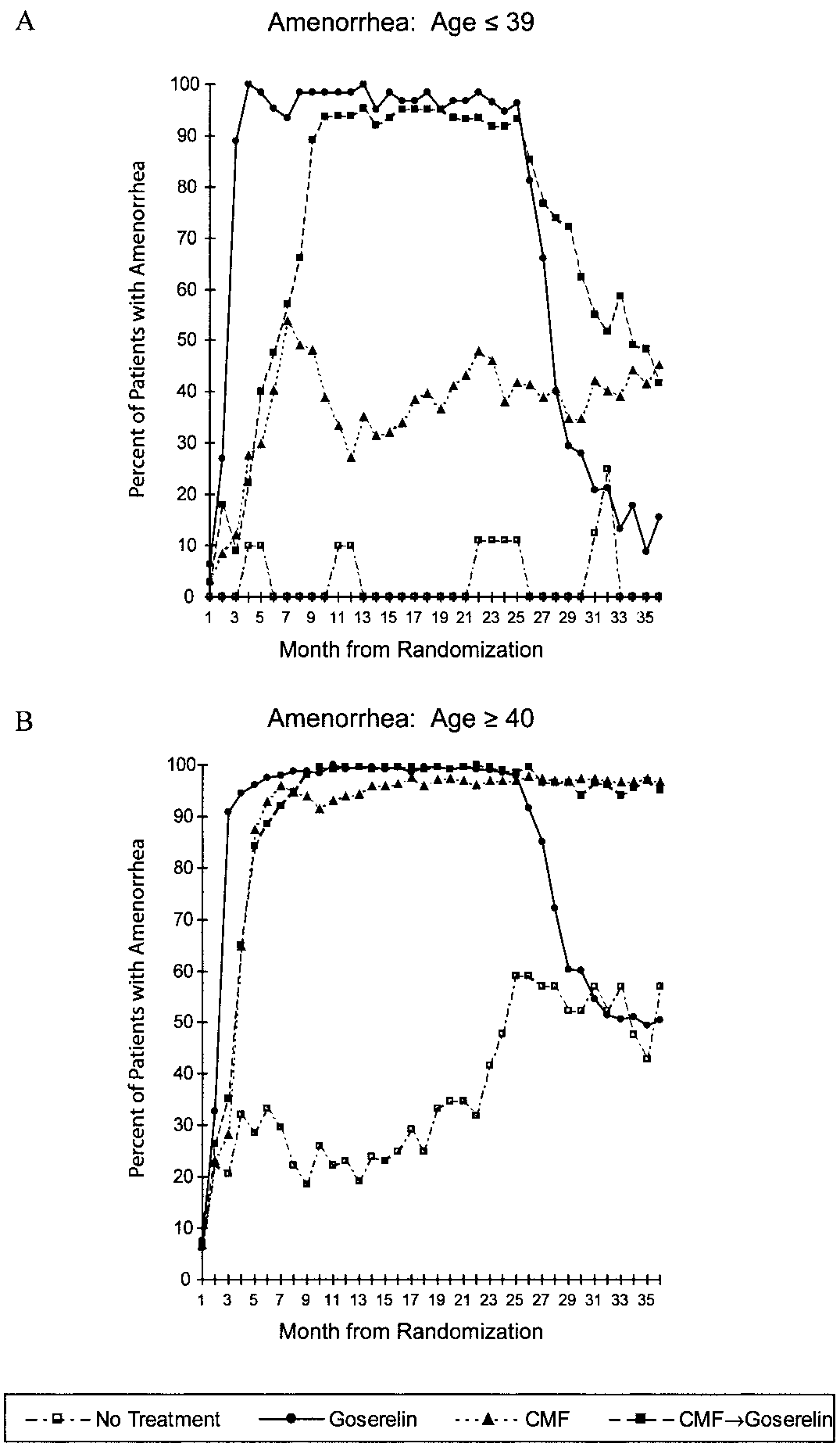 Ovarian function suppression was the first adjuvant systemic
treatment studied for patients with early-stage breast cancer(4,32–34). Chemotherapy is effective adjuvant therapy for pre-menopausal women (6). For several years, the effects of cyto-toxic agents on ovarian function were studied, but the interpre-tation of results remains controversial (7–14). The associationbetween chemotherapy-induced amenorrhea and outcome, how-ever, was confounded in retrospective analyses with chemother-apy dose intensity and duration. Although induction of amenor-rhea was found to be an important indicator of improvedoutcome for chemotherapy regimens that were less dose intenseand of shorter duration (7,8), the effect of amenorrhea on out-come was less evident when an intensive chemotherapy regimenwas used (12). Recently, however, a randomized trial showedstatistically significant increases in both the incidence of amen-orrhea and disease-free survival for very young patients (i.e.,aged 39 years or younger) with ER-positive tumors who re-ceived high-dose chemotherapy with peripheral blood progeni-tor cell support compared with standard doses of chemotherapy(35).
Ovarian function suppression was the first adjuvant systemic
treatment studied for patients with early-stage breast cancer(4,32–34). Chemotherapy is effective adjuvant therapy for pre-menopausal women (6). For several years, the effects of cyto-toxic agents on ovarian function were studied, but the interpre-tation of results remains controversial (7–14). The associationbetween chemotherapy-induced amenorrhea and outcome, how-ever, was confounded in retrospective analyses with chemother-apy dose intensity and duration. Although induction of amenor-rhea was found to be an important indicator of improvedoutcome for chemotherapy regimens that were less dose intenseand of shorter duration (7,8), the effect of amenorrhea on out-come was less evident when an intensive chemotherapy regimenwas used (12). Recently, however, a randomized trial showedstatistically significant increases in both the incidence of amen-orrhea and disease-free survival for very young patients (i.e.,aged 39 years or younger) with ER-positive tumors who re-ceived high-dose chemotherapy with peripheral blood progeni-tor cell support compared with standard doses of chemotherapy(35).