Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Microsoft word - preopformlumbar
SPINE PATIENT QUESTIONNAIRE (Lumbar Attachment)
Please answer all questions completely
It is in your best interest and will assist your
NAME:_______________________________________________________________ DATE: ____________________ BIRTHDATE:__________/__________/__________ HEIGHT:______ FT.______IN. WEIGHT__________LBS A. 1. Referring doctor name and full address:__________________________________________________________
__________________________________________________________________________________________
If not referred, how did you choose this office?____________________________________________________
2. Internist or family doctor name and address:_______________________________________________________
__________________________________________________________________________________________
4. Your age:___________________ Years ________________ Months
6. How long has the pain (or your problem) been present?______________________________________________
7. Has your problem worsened recently? No
Yes – How recently?_________________________________
__________________________________________________________________________________________
8. What started the pain (or problem)?_____________________________________________________________
__________________________________________________________________________________________
B. For patients with NECK OR ARM pain, numbness or weakness:
(If you are seeing the doctor for back or leg pain, go to “C”)
1. What % of your pain is neck pain and what % is arm pain? (check appropriate box)
Neck 10%, Arm 90% Neck 25%, Arm 75%
Neck 60%, Arm 40% Neck 75%, Arm 25%
Arm pain is as follows (check the following):
b. The arm pain is present in the (check the following):
Right: Upper back
Weakness of the (check the following):
6. There is: No numbness of the arms and hands
Numbness of the (check the following):
Right: Upper arm
Forearm Thumb Index finger Long finger Ring finger Small finger
Forearm Thumb Index finger Long finger Ring finger Small finger
is no) difficulty picking up small objects like coins or buttoning buttons.
is no) problem with balance or tripping frequently.
No) headaches in the back of the head. END OF NECK QUESTIONS – PLEASE GO TO “D” C. For patients with BACK OR LEG PAIN, numbness or weakness. (If you are seeing the doctor for neck problems, please complete section “B”)
1. What % of your pain is back pain and what % is leg or buttock pain? (check appropriate box):
Back 10%, Leg 90% Back 25%, Leg 75%
Back 60%, Leg 40% Back 75%, Leg 25%
Leg pain as follows (check the following):
b. The pain is present in the (check the following):
Weakness of the (check the following):
Numbness of the (check the following):
5. The worst position for the pain is: Sitting
6. How many minutes can you stand in one place without pain?
7. How many minutes can you walk without pain?
9. Bending forward: Increases the pain
PLEASE GO TO “D” ALL PATIENTS SHOULD ANSWER THE FOLLOWING
Sometimes increases Does not increase) the pain.
2. There is: No loss of bowel or bladder control
Loss of bowel or bladder control since________________
Not missed any work because of this problem
Missed (how much?) ________________ work
No medicines, therapy, manipulations, injections, or braces
Neck Back
Epidural steroid injections ______ times which
relieved the pain for (how long)?_________________
Trigger point injections _______ times which
relieved the pain for (how long)?_________________
Other:______________________________________
5. List pain medications and dose taken for your spine problem:
6. Previous doctors seen about this problem: None
7. Tests done to evaluate your problem, the dates and the location they were done:
Back #1 DATE #2 DATE WHERE #3 DATE WHERE
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
E. REVIEW OF SYSTEMS: Check all that apply. None apply
Calf cramps w/ walking Frequent urination
Women only: F. MEDICAL HISTORY: Check all that apply.
Ankylosing spondylitis Kidney failure
G. SURGICAL HISTORY: Previous surgeries - List procedures, surgeon and date. OPERATION H. FAMILY HISTORY: Check all that apply. I. MEDICATIONS YOU TAKE:
______________________________________________________________________________________________________________________________________________________________________________________
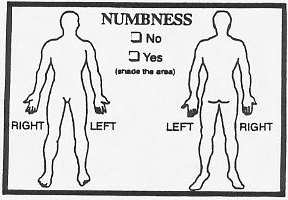
J. ALLERGIES TO MEDICATIONS: No known drug allergies NUMBNESS SOCIAL HISTORY:
1. Work status: Homemaker Retired Disabled On leave
Unemployed Working: __Full time __ Part time
Occupation:____________________________________________
PINS &
__________ packs per day for ________ years.
Quit – When?__________________________ after smoking_______ packs per day for _______ years (total)
Frequently drunk (more than twice a week)
SENSATION
7. Drug overuse/abuse: Never Currently
8. Because of this spine problem, I have filed or plan to file:
Neither a lawsuit or Worker’s Compensation claim
STABBING MY PAIN / DISCOMFORT IS (circle number)
How often do you need to use the following assistive devices?
In the past week, how often have you suffered: (Please circle the number that applies)
A little of A good bit of the time
1. Low back and/or buttock pain…………………. 1
2. Leg pain…………………………………………. 1
3. Numbness or tingling in leg and/or foot………… 1
4. Weakness in leg and/or foot (such as difficulty
lifting foot)……………………………………… 1
In the past week, how bothersome have these symptoms been? (Please circle the number that applies)
5. Low back and/or buttock pain………………
6. Leg pain…………………………………….
7. Numbness or tingling in leg and/or foot…….
difficulty lifting foot)………………………. 1
9. Generally speaking, are your symptoms getting better or worse? (Fill in one circle) The following questions are regarding what you expect from your treatment of your Back/Leg or Neck/Arm Pain. Slightly Somewhat Extremely Slightly Somewhat Extremely Important Important Important Important Important
12. If you had to spend the rest of your life with your back condition as it is right now, how would you feel?
HEALTH STATUS QUESTIONNAIRE (SF-36) Page 1 of 2 The following questions refer to your health in general, including, but not limited to, your back or neck.
1. In general, would you say your health is: (mark only one)
2. Compared to one year ago, how would you rate your health in general now? (mark only one)
The following items are about activities you might do during a typical day. Does your health now limit you in these activities? If so,how much? (Fill in only one circle on each line.)
Yes, Limited Yes, Limited
3. Vigorous activities such as running, lifting
heavy objects or participating in strenuous sports.
4. Moderate activities such as moving a table,
pushing a vacuum cleaner, bowling or golf.
6. Climbing several flights of stairs.
7. Climbing one flight of stairs.
9. Walking more than a mile.
10. Walking several blocks.
11. Walking one block.
During the past 4 weeks, have you had any of the following problems with your work or other regular daily activities as a result of your physical health? (Fill in only one circle on each line.)
13. Cut down on the amount of time you spent on work or other activities.
14. Accomplished less than you would like.
15. Were limited in the kind of work or other activities.
16. Had difficulty performing the work or other activities (e.g. took extra effort)
During the past 4 weeks, have you had any of the following problems with your regular daily activities as a result of any emotional problems (such as feeling depressed or anxious)? (Fill in only one circle on each line.)
17. Cut down the amount of time you spent on work or other activities?
18. Accomplished less than you would like?
19. Didn’t do work or other activities as carefully as usual? HEALTH STATUS QUESTIONNAIRE (SF-36) Page 2 of 2
20. During the past 4 weeks, to what extent has your physical health or emotional problems interfered with your normal social
activities with family, friends, neighbors, or groups? (mark only one)
21. How much bodily pain have you had during the past 4 weeks? (mark only one)
22. During the past 4 weeks how much did pain interfere with your normal work (including both work outside the home and
These questions are about how you feel and how things have been with you during the past 4 weeks. For each question, please give the one answer that comes closest to the way you have been feeling.
How much time during the past 4 weeks… (Fill in only one circle on each line.) A Good Bit A Little of of the Time
the dumps that nothingcould cheer you up?
32. During the past 4 weeks, how much of the time has your physical health or emotional problems interfered with your social
activities (like visiting with friends and relatives, etc.)? (mark only one)
How TRUE or FALSE is each of the following statements for you? (Fill in only one circle on each line.) Definitely Definitely
33. I seem to get sick a little easier than other people.
34. I am as healthy as anybody I know.
35. I expect my health to get worse. OSWESTRY QUESTIONNAIRE
The following questions will give us information as to how your back or leg pain has affected your ability tomanage everyday life. Please answer every section, and mark in each section only the answer which applies toyou. We realize you may consider that two of the statements in any one section relate to you. Please just givethe answer which most clearly describes your problem. Pain Intensity (mark only one) Standing (mark only one)
0. I can stand as long as I want without extra pain.
1. The pain is very mild at the moment.
1. I can stand as long as I want, but it gives me extra pain.
2. The pain is moderate at the moment.
2. Pain prevents me from standing for more than one hour.
3. The pain is fairly severe at the moment.
3. Pain prevents me from standing for more than 1/2 hour.
4. The pain is very severe at the moment.
4. Pain prevents me from standing for more than 10 minutes.
5. The pain is the worst imaginable at the moment.
5. Pain prevents me from standing at all. Personal Care (washing, dressing, etc.) (mark only one) Sleeping (mark only one)
0. I can look after myself normally without causing extra pain.
0. My sleep is never disturbed by pain.
1. I can look after myself normally, but it is very painful.
1. My sleep is occasionally disturbed pain.
2. It is painful to look after myself and I am slow and careful.
2. Because of pain I have less than 6 hours sleep.
3. I need some help, but manage most of my personal care.
3. Because of pain I have less than 4 hours sleep.
4. I need help every day in most aspects of self care.
4. Because of pain I have less than 2 hours sleep.
5. I do not get dressed, wash with difficulty, and stay in bed.
5. Pain prevents me from sleeping at all. Lifting (mark only one) Sex Life (mark only one)
0. I can lift heavy weights without extra pain.
0. My sex life is normal and causes no extra pain.
1. I can lift heavy weights, but it gives me extra pain.
1. My sex life is normal, but causes some extra pain.
2. Pain prevents me from lifting heavy weights off the floor, but
2. My sex life is nearly normal, but is very painful.
I can manage if they are conveniently positioned, e.g. on a table.
3. My sex life is severely restricted by pain.
3. Pain prevents me from lifting heavy weights, but I can manage
4. My sex life is nearly absent because of pain.
light to medium weights if they are conveniently positioned.
5. Pain prevents any sex life at all.
4. I can lift only very light weights. 5. I cannot lift or carry anything at all. Walking (mark only one) Social Life (mark only one)
0. Pain does not prevent me from walking any distance.
0. My social life is normal and gives me no extra pain.
1. Pain prevents me from walking for more than 1 mile.
1. My social life is normal, but increases the degree of pain.
2. Pain prevents me from walking for more than 1/4 mile.
2. Pain has no significant effect on my social life apart from
3. Pain prevents me from walking for more than 100 yards.
limiting my more energetic interest, e.g. sports, etc.
4. I can only walk using a stick or crutches.
3. Pain has restricted my social life and I do not go out as often.
5. I am in bed most of the time and have to crawl to the toilet.
4. Pain has restricted my social life to my home. 5. I have no social life because of pain. Sitting (mark only one) Traveling (mark only one)
0. I can sit in any chair as long as I like.
0. I can travel anywhere without extra pain.
1. I can sit in my favorite chair as long as I like.
1. I can travel anywhere, but it gives me extra pain.
2. Pain prevents me from sitting for more than 1 hour.
2. Pain is bad, but I manage journeys over two hours.
3. Pain prevents me from sitting for more than 1/2 hour.
3. Pain restricts me to journeys of less than one hour.
4. Pain prevents me from sitting for mores than 10 minutes.
4. Pain restricts me to short necessary journeys under 30
5. Pain prevents me from sitting at all.
5. Pain prevents me from traveling except to receive treatment. BACK AND LEG PAIN QUESTIONNAIRE
This form is for the purpose of collecting back pain and leg pain information from you. Answer every question by filling in the appropriate circle. If you are unsure about how to answer a question, please give the best answer you can. Mark only one answer for each question. BACK PAIN
1. On the scale of 0 to 10, mark your intensity of back pain discomfort with 0 being no pain and 10 being pain as bad as it could be. Pain As Bad As It Could Be
2. On the scale of 0 to 10, mark how often you had back pain discomfort with 0 being none of the time and 10
being pain all of the time. All Of The The Time O
1. On the scale of 0 to 10, mark your intensity of leg pain discomfort with 0 being no pain and 10 being pain as bad as it could be. Pain As Bad As It Could Be
2. On the scale of 0 to 10, mark how often you had leg pain discomfort with 0 being none of the time and 10
being pain all of the time. All Of The The Time O HISTORY:
1. Is this an unresolved spinal litigation case?
a. Is this the result of a motor vehicle accident?
b. Is this the result of a personal injury?
c. Other, please describe: ____________________________________
2. How long ago did your current back/neck symptoms begin?
3. Have you had back/neck symptoms before your current episode?
4. How much work did you miss because of your worst prior episode?
O Between 4 and 12 weeks O Between 12 and 24 weeks O More than 24 weeks
5. Have you had previous back/neck surgery?
7. Which health care provider(s) have you used for your current condition? PAIN OR MUSCLE RELAXANT MEDICATION REGIMEN During the last week, how often have you taken the following for your back/leg pain or neck/arm pain:
8. Non-Narcotic medication (such as aspirin, Tylenol, Motrin, Vioxx, Celebrex)
9. Weak narcotic medication (such as Tylenol #3, Darvocet N-100, Darvon, Vicodin)
10. Strong narcotic medication (such as Percodan, Percocet, Morphine, Demerol)
11. Muscle Relaxant medication (such as Flexeril, Parafon Forte, Robaxin)
WORK STATUS:
2. If you are currently working, please answer the following:
c. If you are working less than Full Time or Full Duty, is this because of the problems with your back/neck?
3. If you are not currently working, answer the following:
a. O Are you not working because of problems with your back/neck?
4. Highest level of education attained: O < High School
O Less than one week agoO More than one week but less than three months agoO More than three months but less than six months agoO More than six months but less than one year agoO One to two years agoO More than two years agoO Never employedO Currently working
6. Is your current job the same as when your back/neck problems began?
O Yes, exact same job. O No, job changed due to back problems. O Yes, but job was lightened due to back problems. O No, job changed for reasons other than back. O Not currently working.
7. How long have you been at current job?
8. How much sitting does your job involve?
9. How much standing/walking does your job involve?
10. How often do you lift 25 lbs. on job?
11. How often do you lift 50 lbs. on job?
15. How much do you like your co-workers?
16. How much do you like your supervisor?
17. Other sources of income (mark all that apply)
18. Your opinion of fault (mark all that apply)
19. Financial difficulties due to back condition?
20. Are you on, or planning to apply for Social Security?
21. Are you on, or planning to apply for Disability?
22. Are you on, or planning to apply for Worker’s Compensation?
23. Are you on, or planning to apply for other program?
Other program description __________________________________
____________________________________________________
Términos y Condiciones de Venta de Productos y Servicios Formulario ES104-ES (Rev4) AVISO: La venta de cualquier Producto o Servicio está expresamente condicionada a la aceptación de estos Términos y Condiciones por parte del Comprador. Toda aceptación de la oferta del Vendedor se limita expresamente a la aceptación de estos Términos y Condiciones y el Vendedor rechaza expre
ESUR-guidelines 2005 Printed: 13-04-2006 Page: 1 of 15 ESUR Guidelines on Contrast Media Version 5.0 Content: 1. Renal adverse reactions ESUR guidelines 1.1.To avoid contrast medium induced nephrotoxicity 1.2 Determination of serum creatinine 1.3 Dialysis and contrast media administration 1.4 Administration of contrast media to diabetics taking metformin ESUR Position Statement 1
 SPINE PATIENT QUESTIONNAIRE
SPINE PATIENT QUESTIONNAIRE

 J. ALLERGIES TO MEDICATIONS: No known drug allergies
J. ALLERGIES TO MEDICATIONS: No known drug allergies