Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Granton.gpsurgery.net
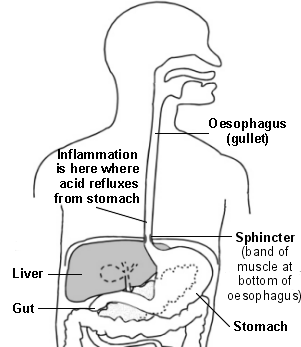
Acid Reflux and Oesophagitis Gastro-Oesophageal Reflux Disease (GORD)
Acid reflux is when acid from the stomach leaks up into the gullet (oesophagus).
This may cause heartburn and other symptoms. A medicine which prevents your
stomach from making acid is a common treatment and usually works well. Some
people take short courses of treatment when symptoms flare up. Some people
need long-term daily treatment to keep symptoms away. Understanding the oesophagus and stomach
When we eat, food passes down the oesophagus (gullet) into the stomach. Cells in the lining of the
stomach make acid and other chemicals which help to digest food. Stomach cells also make
mucus which protects them from damage from the acid. The cells lining the oesophagus are different and have little protection from acid.
There is a circular band of muscle (a 'sphincter') at the junction between the oesophagus and stomach. This relaxes to allow food down, but then normally tightens up and stops food and acid
leaking back up (refluxing) into the oesophagus. In effect, the sphincter acts like a valve.
What are reflux and oesophagitis?
Acid reflux is when some acid leaks up
Oesophagitis means inflammation of the
oesophagitis are due to reflux of stomach
acid which irritates the inside lining of the oesophagus.
The lining of the oesophagus can cope with a certain amount of acid. However, it is more
sensitive to acid in some people. Therefore,
some people develop symptoms with only a small amount of reflux. However, some people
Gastro-oesophageal reflux disease (GORD)
This is a general term which describes the
range of situations - acid reflux, with or without oesophagitis and symptoms. What are the symptoms of acid reflux and oesophagitis?
Heartburn is the main symptom. It is a burning feeling which rises from the upper abdomen
or lower chest up towards the neck. (It is confusing as it has nothing to do with the heart!)
Other common symptoms include: pain in the upper abdomen and chest, feeling sick, an
acid taste in the mouth, bloating, belching, and a burning pain when you swallow hot drinks.
Like heartburn, these symptoms tend to come and go, and tend to be worse after a meal.
Some uncommon symptoms may occur. This makes the diagnosis difficult in some cases
as the symptoms can mimic other conditions. For example:
A persistent cough, particularly at night. This is due to the refluxed acid irritating the
windpipe. Hoarseness or asthma symptoms can sometimes be due to acid reflux.
Severe chest pain develops in some cases (and may be mistaken for a heart attack). What causes acid reflux and who does it affect?
The sphincter at the bottom of the oesophagus normally prevents acid reflux. Problems occur if the sphincter does not work very well. This is common, but in most cases it is not known why it does
not work so well. In some cases the pressure in the stomach rises higher than the sphincter can
withstand. For example, during pregnancy, after a large meal, or when bending forward. If you have a hiatus hernia (when part of the stomach protrudes into the chest through the diaphragm),
you are quite likely to develop reflux. (See separate leaflet called 'Hiatus Hernia'.)
Most people have heartburn at some time, perhaps after a large meal. However, about 1 in 3
adults have some heartburn every few days, and nearly 1 in 10 adults have heartburn at least
once a day. In many cases it is mild and soon passes. However, it is quite common for symptoms
to be frequent or severe enough to affect quality of life. Regular heartburn is more common in smokers, pregnant women, heavy drinkers, the overweight, and those aged between 35 and 64. What tests might be done?
Tests are not usually necessary if you have typical symptoms. Many people are diagnosed with
'presumed acid reflux' when they have typical symptoms, and the symptoms are eased by
treatment. Tests may be advised if symptoms: are severe, or do not improve with treatment, or are not typical of GORD.
Endoscopy is the common test. This is where a thin, flexible telescope is passed down the
oesophagus into the stomach. This allows a doctor or nurse to look inside. With
oesophagitis, the lower part of the oesophagus looks red and inflamed. However, if it looks
normal it does not rule out acid reflux. Some people are very sensitive to small amounts of
acid, and can have symptoms with little or no inflammation to see.
A test to check the acidity inside the oesophagus may be done if the diagnosis is not clear. Other tests such as heart tracings, chest x-ray, etc, may be done to rule out other conditions
What can I do to help with symptoms?
The following are commonly advised. However, there has been little research to prove how well these 'lifestyle' changes help to ease reflux.
Smoking. The chemicals from cigarettes relax the sphincter muscle and make acid reflux
more likely. Symptoms may ease if you are a smoker and stop smoking.
Some foods and drinks may make reflux worse in some people. (It is thought that some
foods may relax the sphincter and allow more acid to reflux.) It is difficult to be certain how
much foods contribute. Let common sense be your guide. If it seems that a food is causing symptoms, then try avoiding it for a while to see if symptoms improve. Foods and drinks that
have been suspected of making symptoms worse in some people include: peppermint,
tomatoes, chocolate, spicy foods, hot drinks, coffee, and alcoholic drinks.
Some medicines may make symptoms worse. They may irritate the oesophagus, or relax
the sphincter muscle and make acid reflux more likely. The most common culprits are anti-
inflammatory painkillers (such as ibuprofen or aspirin). Others include: diazepam,
theophyline, nitrates, and calcium channel blockers such as nifedipine. Tell a doctor if you suspect that a prescribed medicine is making symptoms worse.
Weight. If you are overweight it puts extra pressure on the stomach and encourages acid
reflux. Losing some weight may ease the symptoms.
Posture. Lying down or bending forward a lot during the day encourages reflux. Sitting
hunched or wearing tight belts may put extra pressure on the stomach which may make any
Bedtime. If symptoms recur most nights, it may help to go to bed with an empty, dry
stomach. To do this, don't eat in the last three hours before bedtime, and don't drink in the
last two hours before bedtime. If you raise the head of the bed by 10-15 cms (with books
under the bed's legs), this will help gravity to keep acid from refluxing into the oesophagus.
What are the treatments for acid reflux and oesophagitis? Antacids
These are alkali liquids or tablets that neutralise the acid. A dose usually gives quick relief. There
are many brands which you can buy. You can also get some on prescription. You can use antacids
'as required' for mild or infrequent bouts of heartburn. Acid-suppressing medicines
Two groups of medicines are used - proton pump inhibitors (PPIs) and histamine receptor blockers (H2 antagonists). They work in different ways but both reduce (suppress) the amount of acid that
the stomach makes. PPIs include omeprazole, lansoprazole, pantoprazole, rabeprazole, and
esomeprazole. H2 antagonists include cimetidine, famotidine, nizatidine, and ranitidine. You can
buy some low dose brands at pharmacies. You can use these low dose brands 'as required', or take short courses when you get short bouts of heartburn.
If you get symptoms frequently then see a doctor. You may be advised to take a daily dose of an acid-suppressing medicine to prevent symptoms from occurring. The dose that a doctor prescribes
is usually higher than the dose that you can buy. The treatment plan with acid-suppressing
medicines can vary from person to person.
You may be advised to take a full dose course for a month or so. This often settles
symptoms down and allows any inflammation in the oesophagus to clear. After this, all that
you may need is to go back to antacids 'as required'.
Some people need a course of treatment every now and then when symptoms flare up. Some people need long-term daily acid suppressing treatment. Without medication, their
symptoms return quickly. Long-term treatment is thought to be safe, and side-effects are
uncommon. The aim is to take a full dose course for a month or so to settle symptoms. After this, it is common to 'step-down' the dose to the lowest dose that prevents symptoms.
However, the maximum full dose taken each day is needed in some cases. Prokinetic medicines
These are medicines that speed up the passage of food through the stomach. They include
domperidone and metoclopramide. They are not commonly used but help in some cases, particularly if you have marked bloating or belching symptoms.
This is an option if medicines fail to prevent symptoms, or if you need medication every day to control symptoms. An operation can 'tighten' the lower oesophagus to prevent acid leaking up from
the stomach. It can be done by 'keyhole' surgery, and has a good success rate. Are there any complications from oesophagitis?
Stricture. If you have severe and long-standing inflammation it can cause scarring and
narrowing (a stricture) of the lower oesophagus. This is uncommon.
Barrett's oesophagus. In this condition the cells that line the lower oesophagus become
changed. The changed cells are more prone than usual to become cancerous. (About 1 or 2
people in 100 with Barrett's oesophagus develop cancer of the oesophagus.)
Cancer. Your risk of developing cancer of the oesophagus is slightly increased compared to
the normal risk if you have long-term acid reflux.
It has to be stressed that most people with reflux do not develop any of these complications. Tell
your doctor if you have pain or difficulty (food 'sticking') when you swallow which may be the first
EMIS and PIP 2005 Updated: June 2005 PRODIGY Validated
Comprehensive patient resources are available at www.patient.co.uk
Putting Behind the Pain to Gain Olympic Gold Rowing Canada Aviron and TYLENOL® join forces to get Gold at 2008 Beijing Olympics The road to Olympic Gold is paved with pain, sacrifice, and perseverance. In order to overcome these obstacles and achieve Olympic success, Canadian athletes require a tremendous amount of resources and support. Rowing Canada Aviron is pleased to announce t
The Role of Hypnotherapy in Working With Clutter, which is often related to procrastination, is a leading cause of disorganization. There are many reasons why people clutter. Some reasons include things such as feeling overwhelmed, and your highest priorities at that time, are somewhere else. Perhaps you just don’t know where to start in removing your clutter. How many times have you heard your
 Acid Reflux and Oesophagitis
Acid Reflux and Oesophagitis