Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
030814 methotrexate versus cyclosporine in moderate-to-severe chronic plaque psoriasis
The new england journal of medicine
Methotrexate versus Cyclosporine in Moderate-
Vera M.R. Heydendael, M.D., Phyllis I. Spuls, M.D., Ph.D., Brent C. Opmeer, Ph.D.,
Corianne A.J.M. de Borgie, Ph.D., Johannes B. Reitsma, M.D., Ph.D.,
Wouter F.M. Goldschmidt, M.D., Patrick M.M. Bossuyt, Ph.D.,
Jan D. Bos, M.D., Ph.D., and Menno A. de Rie, M.D., Ph.D. b a c k g r o u n d
Methotrexate and cyclosporine are well-known systemic therapies for moderate-to-
(V.M.R.H., P.I.S., W.F.M.G., J.D.B., M.A.R.)
severe chronic plaque psoriasis. We conduced a randomized, controlled trial comparing
and Clinical Epidemiology and Biostatistics
methotrexate and cyclosporine in terms of effectiveness, side effects, and the quality
(B.C.O., C.A.J.M.B., J.B.R., P.M.M.B.), Ac-ademic Medical Center, University of Am-
sterdam, Amsterdam. Address reprint re-quests to Dr. de Rie at the Department of
Dermatology, Rm. A0-222, Academic Medi-cal Center, University of Amsterdam, P.O.
A total of 88 patients with moderate-to-severe psoriasis were randomly assigned to
treatment for 16 weeks with either methotrexate (44 patients; initial dose, 15 mg per
week) or cyclosporine (44 patients; initial dose, 3 mg per kilogram of body weight per
day) and were followed for another 36 weeks. The primary outcome was the difference
Copyright 2003 Massachusetts Medical Society.
between groups in the psoriasis area-and-severity index after 16 weeks of treatment, af-ter adjustment for base-line values; scores were determined in a blinded fashion bytrained observers.
Two patients were excluded from the analysis after randomization because they werefound to be ineligible, and one patient withdrew his consent. Twelve patients in themethotrexate group had to discontinue treatment because of reversible elevations inliver-enzyme levels, and 1 patient in the cyclosporine group had to do so because of anelevation in the bilirubin level, but all 13 were included in the analysis. After 16 weeksof treatment, the mean (±SE) score for the psoriasis area-and-severity index decreasedfrom 13.4±3.6 at base line to 5.0±0.7 among 43 patients treated with methotrexate,whereas the score decreased from 14.0±6.6 to 3.8±0.5 among 42 patients treated withcyclosporine. After adjustment for base-line values, the mean absolute difference invalues at 16 weeks was 1.3 (95 percent confidence interval, –0.2 to 2.8; P=0.09). Thephysician’s global assessment of the extent of psoriasis, the time to and the rates of re-mission, and the quality of life were similar in the two groups. c o n c l u s i o n s
No significant differences in efficacy were found between methotrexate and cyclospor-ine for the treatment of moderate-to-severe psoriasis.
Downloaded from www.nejm.org at UNIVERSITEITSBIBLIO SZ 215 on September 16, 2003.
Copyright 2003 Massachusetts Medical Society. All rights reserved.
m e t h o t r e x a t e v e r s u s c y c l o s p o r i n e i n m o d e r a t e - t o - s e v e r e c h r o n i c p l a q u e p s o r i a s i s
disease characterized by sharply demarcat-
an estimated worldwide prevalence of 0.1 to 3 per-cent.1 Various therapies are available for the treat-ment of psoriasis, including topical ointments, suchas calcipotriene, corticosteroids, tar, and anthralin;phototherapy with ultraviolet B radiation (UVB) andmethoxsalen (psoralen) with ultraviolet A radiation(PUVA); systemic drugs such as acitretin; and thesystemic immunosuppressant drugs methotrexateand cyclosporine.2,3 Methotrexate and cyclosporineare often used in daily clinical practice, but which ofthe two is more effective has not been established.
The current management of severe psoriasis is
based on the principles of rotational therapy, which
stresses frequent alternations in treatment ap-proaches in order to reduce the cumulative risk ofside effects.4 The choice of treatment is influencedby short-term as well as long-term considerations,including the severity of the disease, the effective-ness of a given medication and its side effects, thepatient’s quality of life, and the ease of treatment. In 1997, a systematic review of the literature showedthat studies of cyclosporine were limited to open,noncomparative, dose-finding, or placebo-con-trolled trials.5 To our knowledge, no comparisonwith methotrexate has been made. According to theguidelines for the treatment of psoriasis, which arebased on the 1997 review, UVB should be tried first,
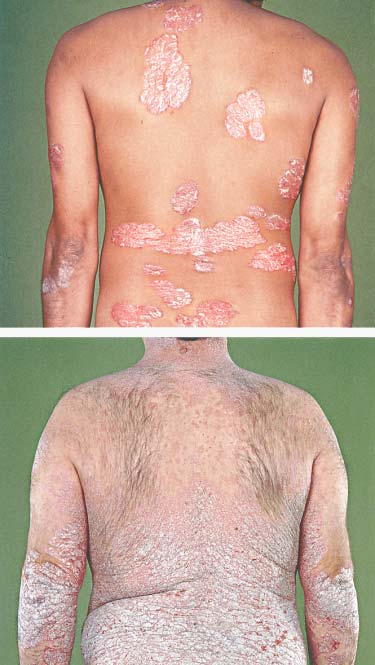
Figure 1. Patient with Moderate-to-Severe Psoriasis, as
and if it proves to be ineffective, it should be fol-
Indicated by a Score of 9.7 on the Psoriasis Area-and- Severity Index (Panel A), and a Patient with Severe
lowed in order by PUVA, methotrexate, acitretin, and
Psoriasis, as Indicated by a Score of 17.1 (Panel B).
finally, cyclosporine.6 We conducted a randomized
Scores for the psoriasis area-and-severity index range
comparison of methotrexate with cyclosporine as
from 0 (no psoriasis) to 72 (the most severe disease
monotherapy for chronic plaque psoriasis, evaluat-
ing side effects, clinical effectiveness, time to andduration of remission, and quality of life.
treated with either methotrexate or cyclosporine. Patients who met any of the following criteria were
excluded: liver or renal impairment; insulin-depend-
p a t i e n t s
ent diabetes mellitus; a high risk of liver-function
Patients were recruited from the Department of abnormalities; a positive serologic test for hepati-Dermatology, Academic Medical Center, Amster- tis B virus; uncontrolled hypertension; a history ofdam, and from local dermatologic centers between cancer, including skin cancer or severe cardiovascu-October 1998 and June 2000. Eligible patients were lar, pulmonary, cerebral, neurologic, or hematolog-18 years of age or older; had moderate-to-severe ic disease; or acute infection requiring antimicrobialchronic plaque psoriasis, defined by a score of at therapy or associated with human immunodefi-least 8 on the psoriasis area-and-severity index ciency virus infection. Patients were also excluded if(a score of 0 indicates the absence of psoriasis, they were pregnant, breast-feeding, or noncompli-and a score of 72 the most severe disease possible) ant with an effective regimen of contraception. (Fig. 1),7 with an insufficient response to topical or
Laboratory tests and ultrasonography of the liv-
UVB therapy (or both); and had not previously been er were performed in all eligible patients. Patients
Downloaded from www.nejm.org at UNIVERSITEITSBIBLIO SZ 215 on September 16, 2003.
Copyright 2003 Massachusetts Medical Society. All rights reserved. The new england journal of medicine
who were treated with methotrexate underwent the treatment, no concomitant antipsoriatic therapy following laboratory tests every two weeks during was permitted, with the exception of emollients. the first month and monthly thereafter until week During the follow-up period, active therapy for pso- 20: a complete blood count and assays of electro- riasis was allowed if necessary, reflecting normal lytes, serum creatinine, blood urea nitrogen, aspar- clinical practice. Drugs known to interfere with pso- tate aminotransferase, alanine aminotransferase, riasis or with the systemic treatments (or with both) alkaline phosphatase, and bilirubin. Patients who were not allowed. were treated with cyclosporine underwent the same laboratory tests according to the same schedule as outcomes well as urinalysis and an assay of magnesium every Effectiveness two months. During the screening period, a test for The score for the psoriasis area-and-severity index hepatitis B virus was also performed in all patients. was the primary outcome measure and was deter- If a relevant abnormality in any of the laboratory val- mined at base line and monthly thereafter by trained ues was noted during treatment, the test was repeat- assessors who were unaware of the treatment as- ed at each visit until the results returned to normal. signments.7 The psoriasis area-and-severity index Patients with moderate or severe steatohepatitis (as combines assessments of psoriasis-induced erythe- established by ultrasonography of the liver) were ma, scaling, and skin thickness, each weighted ac- excluded. The study was approved by the medical cording to the size of the affected area. At each visit, ethics committee at each center.
the physician performed a global assessment, whichis a general evaluation of a patient’s psoriasis, using
a scale of 0 to 10, with a score of 0 indicating the
Eligible patients who had given written informed worst imaginable disease activity and a score of 10consent were randomly assigned on a 1:1 basis to re- the absence of disease activity.11ceive 16 weeks of treatment with either methotrexateor cyclosporine. Randomization was performed Side Effectscentrally with the use of computer-generated ran- We evaluated side effects known to be associateddom numbers and block size of eight patients. The with methotrexate or cyclosporine and effects thatscreening period, during which no active treatment the patient deemed to be relevant to the treatment. for psoriasis was permitted, lasted two weeks for The latter group of side effects was very small. Forpatients who had been receiving topical therapies this reason, we focused our analysis on the firstand four weeks for those who had been receiving group of reported side effects. Side effects that didUVB, PUVA, or systemic drugs. After 16 weeks of not require additional medications, adjustments intreatment, the patients were monitored for another the dose of the study medication, or discontinuation36 weeks. They returned for evaluation every two of the study medication were classified as mild. weeks during the first month of treatment andmonthly thereafter. Quality of LifeWe assessed the patients’ quality of life with use of
t r e a t m e n t r e g i m e n s
the validated Dutch version of the Medical Outcomes
The initial dose of methotrexate was 15 mg per week Study 36-item Short-Form General Health Survey (given in three divided doses with a 12-hour inter- (SF-36).12 The patients completed the SF-36 at base val between doses, according to the schedule of line and every eight weeks thereafter. Summary Weinstein and Frost8), and the initial dose of cyclo- scores were calculated for the physical component sporine was 3 mg per kilogram of body weight per and mental component and were standardized for day (given in two divided doses). After four weeks of the Dutch population; a score of 50 reflects an aver- treatment, the doses were increased, up to 22.5 mg age quality of life in the general population. Scores per week in the case of methotrexate and 5 mg per on each subscale range from 0 (worst) to 100 (best). kilogram per day in the case of cyclosporine, in pa- tients in whom the reduction from base line in the statistical analysis score for the psoriasis area-and-severity index was In the primary analysis, we calculated the difference less than 25 percent. In the event of an adverse ef- between groups in the mean score for the psoriasis fect, the dose could be decreased at any time accord- area-and-severity index after 16 weeks of treatment ing to published guidelines.9,10 During systemic after adjustment for the base-line score using an
Downloaded from www.nejm.org at UNIVERSITEITSBIBLIO SZ 215 on September 16, 2003.
Copyright 2003 Massachusetts Medical Society. All rights reserved.
m e t h o t r e x a t e v e r s u s c y c l o s p o r i n e i n m o d e r a t e - t o - s e v e r e c h r o n i c p l a q u e p s o r i a s i s
analysis of covariance. If a patient missed a visit, we enzyme levels (the highest level measured was anused the score from the previous visit. The physi- alanine aminotransferase level of 198 U per liter). cian’s global assessment score and the quality-of- Treatment was discontinued in one patient in thelife score were analyzed in the same way. In addition, cyclosporine group because of an elevation in thewe used Student’s t-test to compare the percent re- bilirubin level (total bilirubin, 44 mg per deciliterduction from base line in scores for the psoriasis [760 µmol per liter]) and icterus suggestive of thearea-and-severity index in both groups, and we used presence of Gilbert’s syndrome (idiopathic hyper-chi-square tests to compare differences between bilirubinemia). These laboratory abnormalities weregroups in the number of patients reporting side transient, and values returned to normal within foureffects.
to eight weeks after treatment was discontinued. Af-
Differences in the time to reach an almost com- ter cessation of systemic therapy, these 13 patients
plete remission, defined as more than a 90 percent were treated with active therapy for psoriasis, reflect-reduction from base line in the score for the psori- ing normal clinical practice. asis area-and-severity index, and a partial remission,
Neither adjustments of the dose nor discontinu-
defined as more than a 75 percent reduction from ation of the study medication was necessary becausebase line, were compared and tested with the use of of hypertension. Two patients who were receivingthe log-rank test statistic. We calculated the timing cyclosporine (3 mg per kilogram per day) were givenof the return of disease activity (the time to relapse) antihypertensive medication. After the cessation ofand the rate of relapse after oral treatment had been cyclosporine therapy, their blood pressure graduallycompleted in patients with a partial remission. Re- returned to normal and antihypertensive treatmentlapse was defined as a score for the psoriasis area- was stopped. Three patients were already using an-and-severity index that was more than 50 percent of tihypertensive medications before cyclosporine wasthe base-line score or the need for UVB or systemic started, and the regimen was not altered. therapy.
When designing this trial, we calculated that 42 outcomes
patients would be needed in each group for the Effectivenessstudy to have a 95 percent power to rule out a differ- The overall rate of response was high: 94 percentence of two points or more in mean scores for the of all patients had reached the threshold for a min-psoriasis area-and-severity index after a 16-week imal response — a 25 percent reduction from basetreatment period, assuming that the mean (±SE) line in scores for the psoriasis area-and-severity in-expected difference is 0±2.5. We used all available dex — after 12 weeks of treatment, before the doseoutcome data for patients. No interim analyses were was tapered. Figure 3 shows the mean scores forperformed. Two-sided P values of less than 0.05 the psoriasis area-and-severity index during thewere considered to indicate statistical significance. study period. Sixteen weeks after randomization, the
mean (±SE) score was 5.0±0.7 in the methotrexategroup and 3.8
adjustment for base-line values, the mean score
p a t i e n t s
was 1.3 points lower in the cyclosporine group than
Between October 1998 and June 2000, 111 patients in the methotrexate group (95 percent confidencewere screened, 88 of whom underwent randomiza- interval, –0.2 to 2.8; P=0.09). The relative reductiontion (Fig. 2). Three patients were subsequently ex- in the scores from base line to 16 weeks of treat-cluded: two patients had creatinine clearance values ment was 64 percent in the methotrexate group, as(measured according to the method of Cockcroft compared with 72 percent in the cyclosporine group,and Gault13) that were too low, and one patient an absolute difference of 8 percent (95 percent con-withdrew informed consent. Thus, a total of 43 pa- fidence interval, –2 to 18; P=0.14). tients in the methotrexate group and 42 in the cy-
Seventeen patients (40 percent) in the metho-
closporine group were included in the analysis. The trexate group and 14 patients (33 percent) in the cy-base-line characteristics of these patients are shown closporine group had an almost complete remis-in Table 1.
sion (defined as a reduction in the base-line scorefor the psoriasis area-and-severity index of more
l a b o r a t o r y v a l u e s
than 90 percent) during the 16 weeks of treatment
Treatment had to be discontinued in 12 patients in (P=0.55). Partial remission (defined as a reductionthe methotrexate group because of elevated liver in the base-line score of more than 75 percent) was
Downloaded from www.nejm.org at UNIVERSITEITSBIBLIO SZ 215 on September 16, 2003.
Copyright 2003 Massachusetts Medical Society. All rights reserved. The new england journal of medicine
111 Patients with severe plaquepsoriasis assessed for eligibility
Enrollment
6 for PASI <82 for hypertension4 for other reasons
Treatment Period, weeks 0–16 Primary Analysis Follow-up, weeks 17–52 Figure 2. Enrollment, Treatment Assignments, and Reasons for Withdrawal from the Study or Loss to Follow-up.
Scores for the psoriasis area-and-severity index (PASI) range from 0 (no disease) to 72 (the most severe disease possible).
achieved in 26 patients (60 percent) in the metho- (P=0.43 by the log-rank test) or almost completetrexate group and 30 patients (71 percent) in the cy- remission (P=0.34 by the log-rank test) after oralclosporine group (P=0.29). The time needed to treatment was stopped. The median time from thereach an almost complete remission and a partial re- cessation of treatment to the initiation of active ther-mission did not differ significantly between the apy for psoriasis was four weeks in both groups. groups (P=0.70 and P=0.07, respectively, by the log-
After 16 weeks of treatment, there was no sig-
rank test). In four patients in the methotrexate group nificant difference between the two groups in theand in six patients in the cyclosporine group, an in- mean score for the physician’s global assessment. crease in the dose was needed after four weeks of It was 7.0±0.38 in the methotrexate group and 7.8±treatment.
0.29 in the cyclosporine group (absolute difference,
We found no significant differences between 0.9; 95 percent confidence interval, –0.03 to 1.9;
groups in the duration of either partial remission P=0.06).
Downloaded from www.nejm.org at UNIVERSITEITSBIBLIO SZ 215 on September 16, 2003.
Copyright 2003 Massachusetts Medical Society. All rights reserved.
m e t h o t r e x a t e v e r s u s c y c l o s p o r i n e i n m o d e r a t e - t o - s e v e r e c h r o n i c p l a q u e p s o r i a s i s
Side EffectsThe total number of reported side effects was 113
Table 1. Base-Line Characteristics of the Patients.*
in the methotrexate group and 166 in the cyclo-
Methotrexate Cyclosporine
sporine group; side effects were reported by 29 and
35 patients in the two groups, respectively. Signifi-
Characteristic
cantly more patients in the methotrexate group re-
ported nausea (19 of 43, vs. 4 of 42 in the cyclospor-
ine group, P<0.001), whereas more patients in the
cyclosporine group reported headaches (18 of 42,
vs. 7 of 43 in the methotrexate group; P=0.009),
muscle ache (12 of 42 vs. 3 of 43, P=0.007), and par-esthesias in the fingertips and toes (14 of 42 vs. 1 of
43, P<0.001). Additional medication to relieve side
effects was rarely needed in either group. No seri-
ous or irreversible side effects were observed.
No significant differences between the two groups
were found after 16 weeks of treatment in any ofthe subscales of the SF-36. The mean scores for the * Plus–minus values are means ±SE. physical component and the mental component † Scores for the psoriasis area-and-severity index range from 0 (no psoriasis)
to 72 (the most severe disease possible).
were 52±1.7 and 51±1.4 in the methotrexate group,respectively, and 53±1.4 and 51±1.4 in the cyclo-sporine group, respectively. After adjustment forbase-line values, the estimated absolute differencein scores between the methotrexate and cyclospor-
ine groups for the physical and mental components
Treatment Follow-up
was –0.8 (95 percent confidence interval, –4.6 to3.0; P=0.69) and –0.5 (95 percent confidence inter-
val, –3.9 to 2.9; P=0.75), respectively. PASI Score
In this randomized trial of two frequently used sys-
temic treatments in patients with moderate-to-severechronic plaque psoriasis, we found that methotrex-ate and cyclosporine were similarly effective. In both
groups, scores for the psoriasis area-and severity in-
Weeks after Randomization
dex started to decrease once treatment was begun. No. Evaluated
After 16 weeks of treatment, the mean adjusted ab-
solute difference between the groups was small:
Figure 3. Mean (±SE) Scores for the Psoriasis Area-and-Severity Index (PASI)
We conducted this study according to interna-
during Treatment and Follow-up.
tional guidelines that have been developed for both
A score of at least 8 was used as an inclusion criterion.
treatments.9,10 Despite the existence of these guide-lines, the regimens of both methotrexate and cyclo-sporine vary substantially among countries in termsof the route (oral vs. intramuscular) and the dose. initial dose of 2.5 to 5 mg because of the risk of my-We used a starting dose of 15 mg of methotrexate elosuppression during the first 10 days of treat-per week. We chose this dose in the absence of evi- ment.9 In accordance with the guidelines,10 the dosedence from dose-finding and treatment-duration of cyclosporine could be increased after four weeksstudies. The guidelines, however, recommend an in the event of an insufficient response (less than
Downloaded from www.nejm.org at UNIVERSITEITSBIBLIO SZ 215 on September 16, 2003.
Copyright 2003 Massachusetts Medical Society. All rights reserved. The new england journal of medicine
a 25 percent decrease in the score on the psoriasis deficiency. Whether methotrexate-induced eleva-area-and-severity index from base line). The 16-week tions in liver enzymes can be reduced by folate sup-treatment period we used was proved to be effective plementation is heavily debated, and was not an-in a previous study of cyclosporine, in which more swered in a recently completed Cochrane review,than 80 percent of the study population had clinical owing to a lack of uniformity in outcome meas-improvement.14 Ho et al.15 demonstrated that ta- ures.19 A randomized, controlled trial involving pa-pering the dose of cyclosporine, rather than abrupt- tients with rheumatoid arthritis showed that thely stopping treatment, does not increase the time to incidence of hepatotoxicity during methotrexaterelapse. Since these results were not available when treatment was significantly lower in the group treat-we initiated our study, we tapered the dose during ed with folate than in the placebo group.20 Sincethe last four weeks of treatment.
folate supplementation does not cause severe side
Both treatments for moderate-to-severe psoria- effects and is not expensive, we now prescribe it for
sis are readily available, and there is ample evidence our patients who are taking methotrexate. of their effectiveness from placebo-controlled stud-
We demonstrated that the effectiveness and tol-
ies and uncontrolled studies. Our results of the ef- erability of methotrexate are similar to those of cy-fectiveness of cyclosporine are in agreement with closporine in patients with moderate-to-severe pso-those of earlier studies.16,17
riasis. Differences between the treatments in terms
Overall, the tolerability of both drugs was good. of side effects, long-term adverse effects, ease of ad-
Only one patient in the cyclosporine group had to ministration (once-daily vs. twice-daily treatment),discontinue treatment because of an adverse effect and costs can be used to guide treatment decisions— an elevation in bilirubin. Twelve patients had to in individual cases. discontinue methotrexate treatment, all because of
Supported by a grant (OG 97-009) from the Dutch Health Au-
elevations in liver enzymes. These elevations were thorities.
We are indebted to the patients who participated in the study; to
mild, and all values returned to normal within four Leonard Witkamp, M.D., Ph.D., for the idea for this study; to Gabriëlleto eight weeks after treatment had been discontin- A.M. Appel, Fridolijn Langenhuijsen-Jongevos, M.D., Femke M.C. ued. Liver enzyme elevations during methotrexate Mombers, Yolanda Remmelzwaal, and Henry J.C. de Vries, M.D.,
Ph.D., for determining the psoriasis area-and-severity index scores;
treatment have been well documented.18 Most of the to Jantien A. Manders, M.P.A., for financial management of the study;side effects observed immediately after the receipt to our fellow dermatologists for referring patients; to Ineke Tenof methotrexate (abdominal discomfort, oral ulcer- Berge, M.D., Ph.D., for her advice on safety monitoring; to John
de Korte for his expertise on the quality-of-life assessment; and to the
ations, and cytopenias) resemble the effects of folate Department of Radiology for conducting the liver ultrasonography. r e f e r e n c e s
populations. J Clin Epidemiol 1998;51:1055-
study of psoriasis with emphasis on quality
riasis — oral therapy with a new retinoid.
of life assessment. Dermatol Clin 1996;14:
13. Cockcroft DW, Gault MH. Prediction of
creatinine clearance from serum creatinine.
psoriasis: a new therapeutic schedule. Arch
asis. 1. Topical therapy and phototherapy. 14. Ho VC, Griffiths CEM, Albrecht G, et al.
Intermittent short courses of cyclosporin
Idem. Treatment of psoriasis. 2. Systemic
HI, Weinstein GD. Methotrexate in psoria-
(Neoral) for psoriasis unresponsive to topi-
therapies. J Am Acad Dermatol 2001;45:649-
sis: revised guidelines. J Am Acad Dermatol
cal therapy: a 1-year multicentre, randomised
study. Br J Dermatol 1999;141:283-91. 10. Lebwohl M, Ellis C, Gottlieb A, et al. 15. Ho VCY, Griffiths CEM, Berth-Jones J,
to the treatment of moderate to severe psori-
et al. Intermittent short courses of cyclospor-
asis with rotational therapy. J Am Acad Der-
emphasis on the treatment of psoriasis. J Am
agement of psoriasis: a 2-year cohort study. 11. Chaudhari U, Romano P, Mulcahy LD,
JD. A systematic review of five systemic treat-
Dooley LT, Baker DG, Gottlieb AB. Efficacy
16. Berth-Jones J, Henderson CA, Munro CS,
ments for severe psoriasis. Br J Dermatol
et al. Treatment of psoriasis with intermittent
plaque-type psoriasis: a randomised trial.
short course cyclosporin (Neoral): a multi-
center study. Br J Dermatol 1997;136:527-30.
JJE, Witkamp L, Bos JD. The development of
12. Aaronson NK, Muller M, Cohen PD, et al. 17. Griffiths CEM, Powles AV, McFadden J,
practice guidelines for the treatment of severe
Translation, validation, and norming of the
Baker BS, Valdimarsson H, Fry L. Long-term
plaque form psoriasis. Arch Dermatol 1998;
Dutch language version of the SF-36 Health
cyclosporin for psoriasis. Br J Dermatol 1989;
Downloaded from www.nejm.org at UNIVERSITEITSBIBLIO SZ 215 on September 16, 2003.
Copyright 2003 Massachusetts Medical Society. All rights reserved.
m e t h o t r e x a t e v e r s u s c y c l o s p o r i n e i n m o d e r a t e - t o - s e v e r e c h r o n i c p l a q u e p s o r i a s i s
18. Wollina U, Ständer K, Barta U. Toxicity
folinic acid for reducing side effects in
in rheumatoid arthritis: a forty-eight week,
of methotrexate treatment in psoriasis and
patients receiving methotrexate for rheuma-
multicenter, randomized, double-blind, pla-
psoriatic arthritis — short- and long-term
toid arthritis. Cochrane Database Syst Rev
cebo-controlled study. Arthritis Rheum 2001;
toxicity in 104 patients. Clin Rheumatol 2001;
20. van Ede AE, Laan RFJM, Rood MJ, et al. Copyright 2003 Massachusetts Medical Society.19. Ortiz Z, Shea B, Saurez Almazor M,
Effect of folic or folinic acid supplementation
Moher D, Wells G, Tugwell P. Folic acid and
on the toxicity and efficacy of methotrexate
Downloaded from www.nejm.org at UNIVERSITEITSBIBLIO SZ 215 on September 16, 2003.
Copyright 2003 Massachusetts Medical Society. All rights reserved.
UBERMORGEN.COM (lizvlx/Hans Bernhard) Lilly controls my Foriginals For their first Italian personal exhibition, the Austrian artist duo UBERMORGEN.COM (lizvlx/Hans Bernhard) is showing a synthesis of their recent work -- a subtle membrane connecting the digital and the biological: a mix that UBERMORGEN.COM, an identity that lives and works on the Net, experienced on their own bodies. One o
Revista Philosophica Vol. 29 [Semestre I / 2006] Valparaíso (287 - 303) E L C O N O C I M I E N T O D I V I N O D E L O S A C T O S F U T U R O S E N B Á Ñ E Z , M O L I N A , S U Á R E Z Y B R I C E Ñ O 1 The Divine Knowledge of Future Acts in Báñez, Molina, Suárez and Briceño MIRKO SKARICA Profesor Extraordinario, Instituto de Filosofía, Pontifi
 m e t h o t r e x a t e v e r s u s c y c l o s p o r i n e i n m o d e r a t e - t o - s e v e r e c h r o n i c p l a q u e p s o r i a s i s
disease characterized by sharply demarcat-
an estimated worldwide prevalence of 0.1 to 3 per-cent.1 Various therapies are available for the treat-ment of psoriasis, including topical ointments, suchas calcipotriene, corticosteroids, tar, and anthralin;phototherapy with ultraviolet B radiation (UVB) andmethoxsalen (psoralen) with ultraviolet A radiation(PUVA); systemic drugs such as acitretin; and thesystemic immunosuppressant drugs methotrexateand cyclosporine.2,3 Methotrexate and cyclosporineare often used in daily clinical practice, but which ofthe two is more effective has not been established.
m e t h o t r e x a t e v e r s u s c y c l o s p o r i n e i n m o d e r a t e - t o - s e v e r e c h r o n i c p l a q u e p s o r i a s i s
disease characterized by sharply demarcat-
an estimated worldwide prevalence of 0.1 to 3 per-cent.1 Various therapies are available for the treat-ment of psoriasis, including topical ointments, suchas calcipotriene, corticosteroids, tar, and anthralin;phototherapy with ultraviolet B radiation (UVB) andmethoxsalen (psoralen) with ultraviolet A radiation(PUVA); systemic drugs such as acitretin; and thesystemic immunosuppressant drugs methotrexateand cyclosporine.2,3 Methotrexate and cyclosporineare often used in daily clinical practice, but which ofthe two is more effective has not been established.