Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Jcojournal.org
Gettinger et al 3. Doorn RV, Kirtschig G, Scheffer E, et al: Follicular and epidermal
epidermis and epidermal appendages. J Invest Dermatol 83:385-393,
alterations in patients treated with ZD1839 (Iressa), an inhibitor of the
epidermal growth factor receptor. Br J Dermatol 147:598-601, 2002
7. Jost M, Kari C, Rodeck U: The EGF receptor, an essential regulator of 4. Boucher KW, Davidson K, Mirakhur B, et al: Paronychia induced by
multiple epidermal functions. Eur J Dermatol 10:505-510, 2000
cetuximab, an antiepidermal growth factor receptor antibody. J Am Acad
8. Albanell J, Rojo F, Averbuch S, et al: Pharmacodynamic studies of the
epidermal growth factor receptor inhibitor ZD1839 in skin from cancer
5. Monti M, Mancini LL, Ferrari B, et al: Cutaneous toxicity induced by
patients: Histopathologic and molecular consequences of receptor inhibi-
cetuximab. J Clin Oncol 21:4651-4653, 2003
6. Nanney LB, Magid M, Stoscheck CM, et al: Comparison of epider-
mal growth factor binding and receptor distribution in normal human
CASE 2. Scrotal Ulceration During All-Trans-
A 33-year-old white man with no significant past
medical history presented with fatigue and painful gin-gival bleeding. Initial laboratory studies revealed pancy-topenia with a WBC count of 1,100 cells/L, hemoglobinlevel of 6.9 g/dL, and platelet count of 36,000 cells/L. Prothrombin time was 16.7 seconds (normal, 11.6 to 14.4seconds), activated partial thromboplastin time was 36.6seconds (normal, 23 to 35 seconds), fibrinogen was 145mg/dl (normal, 180 to 400 mg/dl), and fibrin split prod-ucts were greater than 80 g/ml (normal, Ͻ 10 g/ml). Review of the peripheral smear showed occasional pro-myelocytes with Auer rods. Subsequent bone marrow
aspirate and biopsy confirmed the diagnosis of acutepromyelocytic leukemia (APL), with cytogenetic analysisrevealing presence of the t(15;17) translocation. All-
phase of his treatment given for 2 weeks every 3 months.1
trans-retinoic acid (ATRA) therapy was initiated at 45
Scrotal ulceration did not recur with the reintroduction
mg/m2 divided in two daily doses, with the introduction
of ATRA. He remains in molecular remission 21 months
of induction chemotherapy with idarubicin and cytara-
after the initial diagnosis with undetected promyelocytic
bine 3 days later. Shortly after starting ATRA, the patient
leukemia/retinoic acid receptor-␣ transcripts by reverse
developed fevers as high as 105°F (40.5°C). These fevers
transcriptase polymerase chain reaction.
were ultimately attributed to ATRA after an extensive
The introduction of ATRA, a vitamin A derivative,
evaluation that included multiple blood cultures. Fevers
has revolutionized the treatment and survival of patients
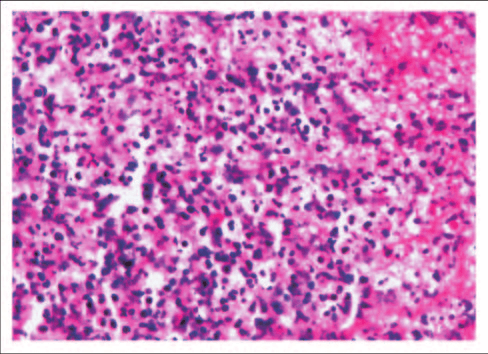
persisted throughout ATRA treatment. The patient didnot have pulmonary complaints or leukocytosis sugges-tive of retinoic acid-APL syndrome. On the 30th day ofATRA therapy, the patient developed a 1.5-cm painless,dusky, nonpruritic and superficial scrotal ulcer (Fig 1). ATRA was discontinued and the patient defervescedwithin 12 hours of stopping the medication. Superficialcultures of the ulcer grew Pseudomonas and Enterococcus,believed to be superimposed bacterial infection. Biopsyrevealed a dense neutrophilic infiltrate and tissue necro-sis with negative acid fast, periodic acid-Schiff, and Gro-cott’s methenamine silver stains for microorganisms (Fig2). The ulcer gradually resolved during the 2 weeks afterdiscontinuing ATRA. Our patient achieved a completecytogenetic and molecular remission after inductionchemotherapy. He received consolidation chemother-apy, and ATRA was resumed during the maintenance
Downloaded from jco.ascopubs.org on March 9, 2014. For personal use only. No other uses without permission.
Copyright 2004 American Society of Clinical Oncology. All rights reserved. Diagnosis in Oncology
diagnosed with APL. By inducing maturation and subse-
sion might already have been achieved. Scrotal ulceration has
quent apoptosis of APL cells, ATRA therapy alone has led
not recurred with six cycles of ATRA maintenance therapy.
to complete remissions, albeit brief. Further induction,
Scott Gettinger, Ilan Shapira, and Noah Scheinfeld
consolidation, and maintenance chemotherapy is needed
Beth Israel Medical Center, New York, NY; and The Albert Einstein
to sustain remissions. ATRA treatment is generally well-
tolerated, with side effects including fever, headache, dry
Michael Grossbard
skin, xerostomia, cheilitis, arthralgia, and hyperlipid-
Beth Israel Medical Center; St Luke’s-Roosevelt Hospital Center; and
emia. A more serious complication is the potentially
Columbia University College of Physicians and Surgeons, New York, NY
life-threatening retinoic acid-APL syndrome, character-
2004 by American Society of Clinical Oncology
ized by hyperleukocytosis, fever, dyspnea, radiographicpulmonary infiltrates, pleural and/or pericardial effu-
Authors’ Disclosures of Potential
sions, renal failure, and weight gain.2 We describe a case
Conflicts of Interest
of scrotal ulceration with ATRA use, an occurrence that
The authors indicated no potential conflicts of interest.
has been rarely reported in the medical literature.3-10
REFERENCES
Scrotal lesions secondary to ATRA use have been
1. Tallman M, Nabhan C, Feusner J, et al: Acute promyelocytic leukemia:
Evolving therapeutic strategies. Blood 99:759-767, 2002
described in both the setting of treatment for APL3-9 and
2. Frankel SR, Eardly A, Lauwers G, et al: The “retinoic acid syndrome”
during combined therapy with interferon in a phase II
in acute promyelocytic leukemia. Ann Intern Med 117:292-296, 1992
trial for advanced non–small-cell lung carcinoma.10 Case
3. Sun GL: Treatment of acute promyelocytic leukemia (APL) with
all-trans retinoic acid (ATRA): A report of five-year experience. Chung Hua
reports indicate that such ulcerations are usually accom-
panied by fever and often occur with recovering WBC. 4. Tajima K, Sagae M, Yahagi A, et al: Scrotal exfoliative dermatitis with
The exact pathogenesis is uncertain but may involve
ulcers associated with treatment of acute promyelocytic leukemia duringtreatment with all-trans retinoic acid. Rinsho Ketsueki 39:48-52, 1998
cytokine release7,11,12 and/or superoxide production12
5. Goto H, Tsurumi H, Kasahara S, et al: Acute promyelocytic leukemia
leading to leukocyte activation and subsequent tissue
accompanied by scrotal Fournier’s gangrene during ATRA treatment and
damage. The ulcers typically resolve shortly after discon-
relapsed as external ear tumor. Rinsho Ketsueki 39:1169-1174, 1998
6. Levy V, Jaffarbey J, Aouad K, et al: Fournier’s gangrene during
tinuation of ATRA. Another entity that might be consid-
induction treatment of acute promyelocytic leukemia, a case report. Ann
ered in our case is acute febrile neutrophilic dermatosis,
7. Mori A, Tamura S, Katsuno T, et al: Scrotal ulcer occurring in patients
or Sweet’s syndrome, which is often associated with he-
with acute promyelocytic leukemia during treatment with all-trans retinoic
matologic malignancies. However, pathology did not re-
veal the characteristic nodular dense perivascular
8. Charles KS, Kanaa M, Winfield DA, et al: Scrotal ulceration during
all-trans retinoic (ATRA) therapy for acute promyelocytic leukaemia. Clin Lab
neutrophilic infiltrates and neutrophilic karyorrhexis. In
addition, our patient did not have peripheral leukocyto-
9. Esser AC, Nossa R, Shoji T, et al: All-trans-retinoic acid-induced scrotal
sis at the onset of the cutaneous lesion.
ulcerations in a patient with acute promyelocytic leukemia. J Am AcadDermatol 43:316-317, 2000
Considering the profound benefit of ATRA therapy, it is
10. Athanasiadis I, Kies MS, Miller M, et al: Phase II study of all-trans-
reasonable to consider continuing ATRA therapy when scro-
retinoic acid and alpha-interferon in patients with advanced non-small celllung cancer. Clin Cancer Res 1:973-979, 1995
tal ulceration develops. Topical corticosteroids and anti-
11. Degos L, Dombret H, Chomienne C, et al: All-trans-retinoic acid as a
biotic ointment to prevent superimposed infection have
differentiating agent in the treatment of acute promyelocytic leukemia.
been used to manage the ulceration and might be bene-
12. Koga H, Fujita I, Miyazaki S: Effects of all-trans retinoic acid on
ficial. We chose to temporarily discontinue ATRA be-
superoxide generation in intact neutrophils and a cell-free system. Br J
cause our patient was also having high fevers believed to
be secondary to ATRA, and we felt that a complete remis-
barbiturate-based therapy (oral phenobarbital 100 mg daily)
CASE 3. Toxic Epidermal Necrolysis Induced
for prevention of epileptic attacks was started. In addition,
whole-brain radiotherapy (50 Gy) was completed 2 days be-fore hospital admission. On physical examination, there was a
A 51-year-old woman with metastatic breast cancer
generalized erythema over the whole body. Bullous lesions and
including brain and lung metastases was admitted to our
some morbilliform target lesions appeared on her neck, trunk,
hospital because of recent appearance of bullous urticari-
and distal extremities. Finally, sheet-like loss of epidermis and
oid lesions, severe stomatitis, and radiotherapy-induced
raised flaccid blisters that spread with pressure occurred, and
burns along the scalp, involving the top of the ears.
Nikolsky’s sign (ie, dislodgment of epidermis by lateral pres-
Forty-five days earlier, brain metastases were diagnosed and
sure) was positive on erythematous areas. With trauma,
Downloaded from jco.ascopubs.org on March 9, 2014. For personal use only. No other uses without permission.
Copyright 2004 American Society of Clinical Oncology. All rights reserved.
N Scale Weathering: Concepts and Techniques N SCALE WEATHERING: CONCEPTS & TECHNIQUES Concepts: The weathering of N Scale locos and rolling stock requires some unique thinking in order to achieve realistic results. There are plenty advantages of weathering in N Scale and I will try to demonstrate how we can use these to improve the overall appearance of N scale locos and rolling stock to
The Practical Use of Cannabinoids in the Dr Willy Notcutt, FRCA, FFPMRCA James Paget Hospital GREAT YARMOUTH, Norfolk, UK william.notcutt@jpaget.nhs.uk • The endocannabinoid system is a therapeutic target yet to be properly explored for pain management • Cannabinoids are a new medicine to clinicians– New role, effects, benefits, side-effectsBut…• Many of our patient

 Gettinger et al
Gettinger et al