Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Metrc.smu.edu.cn
Am. J. Trop. Med. Hyg., 79(4), 2008, pp. 568–570Copyright 2008 by The American Society of Tropical Medicine and Hygiene
Case Report: A Severe Eosinophilic Meningoencephalitis Caused by Infection of
Hua Li, Feng Xu, Jin-Bao Gu, and Xiao-Guang Chen*
Department of Parasitology, School of Public Health and Tropical Medicine, Southern Medical University, Guangzhou, China;Department of Neurological Internal Medicine, Wuyi Traditional Chinese Medical Hospital, Jiangmen, China
This paper reports a severe case of eosinophilic meningoencephalitis after infection with Angiostrongylus
On Hospital Day 13, a bone marrow test showed eosinophilia.
A second CSF test showed an opening pressure of 38 cm H O,
Angiostrongylus cantonensis is prevalent in the Pacific is-
199 WBCs (48% neutrophils, 22% lymphocytes, 30% eosino-
lands and Southeast Asia and the most common cause of
phils), 4 red blood cells (RBCs), and protein 398 mg/dL. CSF
eosinophilic meningitis/meningoencephalitis in humans living
was clear, and culture for bacteria yielded no growth. A pe-
in endemic regions.1 Snails and slugs are the major interme-
ripheral blood smear suggested eosinophile granulocytes
diate hosts in which first-stage larvae develop to infective
Յ 12%. Given the presence of an eosinophilic pleocytosis in
third-stage larvae. Humans become infected through the con-
the CSF, bone marrow and peripheral blood, parasitic infec-
sumption of raw snails, fresh water or vegetables contami-
tion of the central nervous system was suspected, but the
nated with intermediate or carrier hosts. Third-stage larvae
are transported to the central nervous system, where they
On Hospital Day 14, the patient’s condition worsened. He
incite eosinophilic meningitis/meningoencephalitis with
became unconscious and developed hyperpyrexia and neck
symptoms including headache, fever, and neck stiffness. We
rigidity. The patient history showed that on August 1, accord-
present here a severe case of eosinophilic meningoencepha-
ing to a folk prescription, the patient ate two raw golden apple
litis after infection with A. cantonensis.
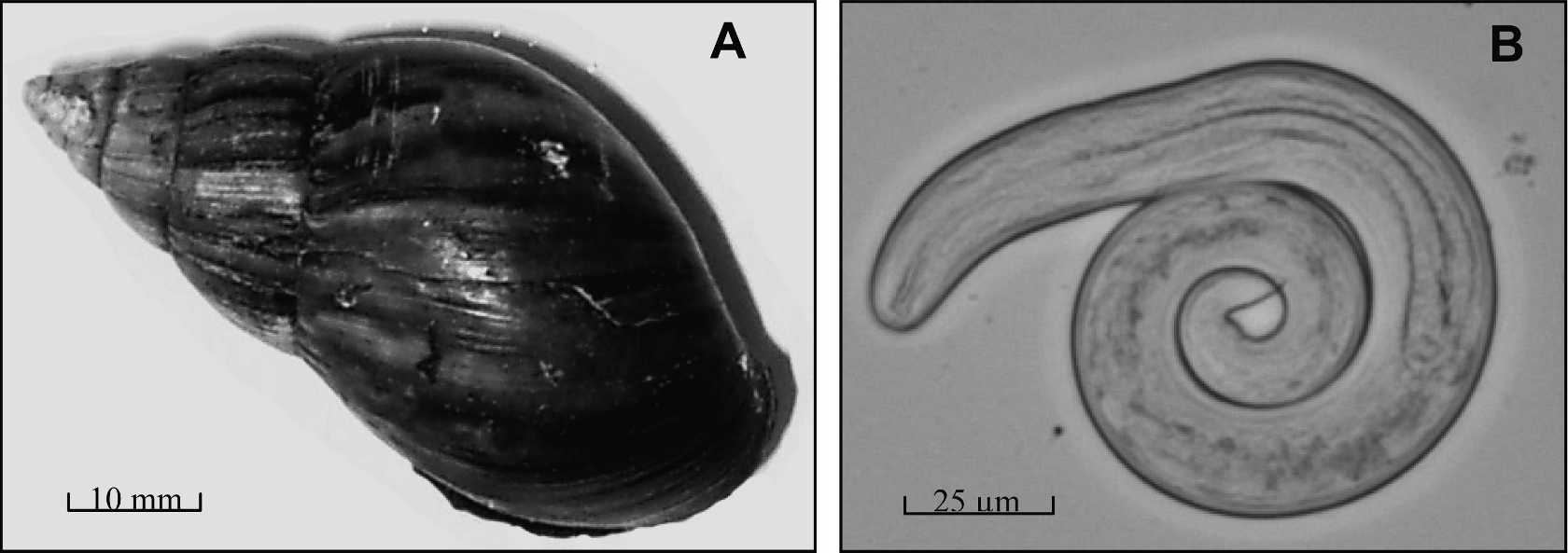
snails (A. canaliculatus) to treat his insomnia. An ELISAshowed that both his serum and CSF were positive for anti-bodies (IgG and IgM) against A. cantonensis, as well as para-
site-circulating antigen. A. cantonensis larvae also were de-tected in snails collected from the same region where the
A 23-year-old man presented to our hospital on August 5,
patient had consumed uncooked snails (Figure 1). Based on
2006, after the onset of severe abdominal pain, nausea, vom-
the history, clinical manifestations, and laboratory tests, an-
iting, and weakness for 3 days and lower limb pain and po-
giostrongyliasis was suspected, and albendazole was used for
dalgia for 1 day before admission. On admission, he was con-
scious and oriented. The findings of a physical examination
On Hospital Day 19, the patient exhibited symmetric and
were unremarkable. No obvious focal neurologic signs were
ascending weakness, quadriparesis, areflexia, and type I re-
detected. Laboratory tests showed a blood leukocyte count of
spiratory failure. Muscle atrophy was observed in the limbs
15,700/mm3, with 81.7% neutrophils. Results of urine and
and most obviously in the hands. A third CSF analysis showed
350 WBCs (23% neutrophils, 55% lymphocytes, 22% eosino-
On Hospital Day 2, the patient developed an irregular low-
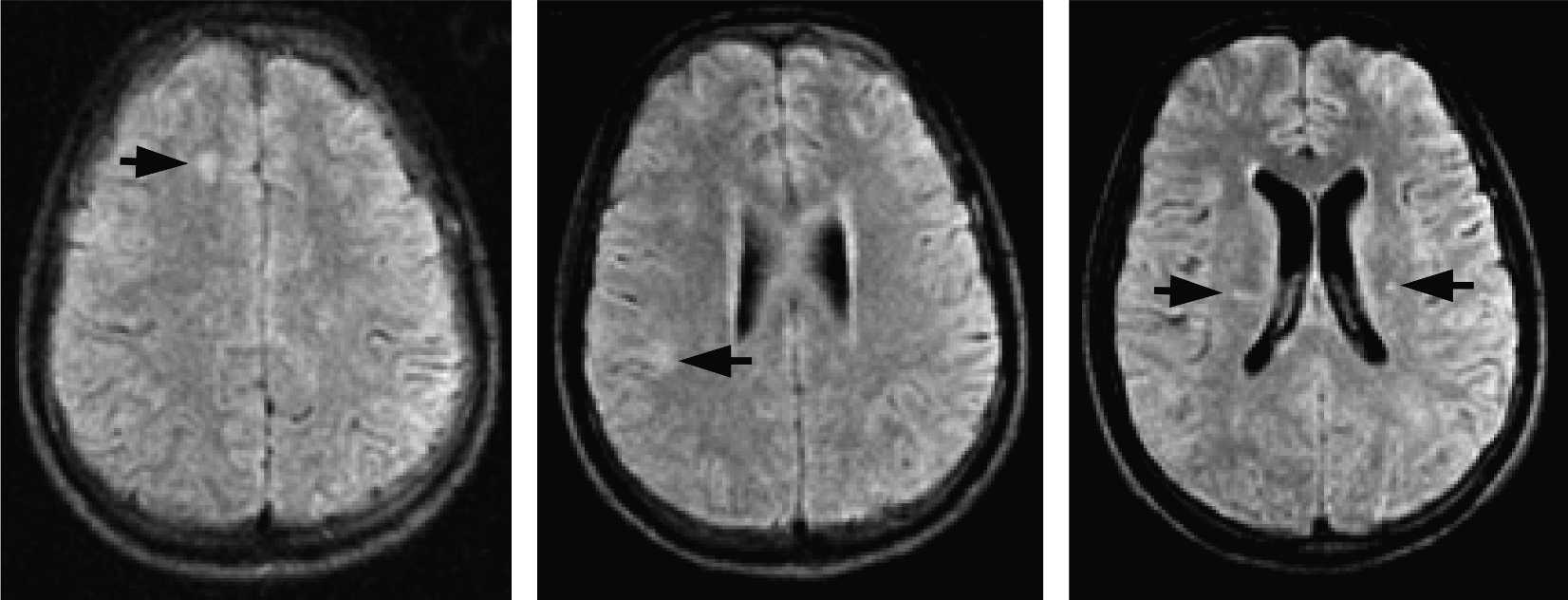
phils), 2 RBCs, and a protein level of 905 mg/dL. Magnetic
grade fever and was administered anti-inflammatory and
resonance imaging (MRI) of the pars encephalica showed
symptomatic treatment. After treatment, the patient experi-
many inflammatory foci in the ambi-temporal lobes and left
enced a decrease in abdominal distention and pain but a
cerebellum (Figure 2); however, abnormalities in spinal cord
and nerve roots were not observed. The patient’s history,
On Hospital Day 9, the patient’s condition suddenly wors-
characteristic symptoms and signs of meningoencephalitis,
ened. He had a severe headache with cognitive impairment
presence of eosinophilic pleocytosis, and detection of specific
and slowed reactions. Body temperature reached 39.5°C.
antibodies and antigens of A. cantonensis resulted in a diag-
Blood test showed hyponatremia and hypochloremia. A ce-
nosis of a severe eosinophilic meningoencephalitis after in-
rebral spinal fluid (CSF) lumbar puncture test showed an
opening pressure of 32 cm H O, 290 white blood cells
The patient was transferred to the intensive care unit
(WBCs) (30% neutrophils and 70% lymphocytes), protein
(ICU), and a combined therapy was applied that included a
262 mg/dL, glucose 2.23 mmol/L, and chlorine 104.4 mmol/L.
respiratory machine to assist breathing, a high dose of dexa-
No space-occupying lesions or other abnormalities were
methasone as an anti-inflammtory (20 mg, four times a day),
found by computer-assisted tomography of the brain.
␥-globulin to increase the patient’s immunity (0.5 g/kg), 20%mannitol to decrease the intracranial pressure, and Chineseherbs (Xing Nao Wan) to recover the function of nerve cells. The patient’s condition improved quickly with this treatment
* Address correspondence to Xiao-Guang Chen, Department of
and he became conscious 2 days later. After 4 months of
Parasitology, School of Public Health and Tropical Medicine, South-
treatment, the patient recovered and was discharged from the
ern Medical University, Guangzhou GD 510515, China. E-mail:xgchen@fimmu.com
EOSINOPHILIC MENINGOENCEPHALITIS WITH A. CANTONENSISA, An A. canaliculatus (golden apple snail) collected from the place where the patient found the consumed snail. B, A third-stage
larva of A. cantonensis separated from an infected A. canaliculatus.
which is more difficult to sample for diagnosis, and the para-sitic larvae are small in size and often adhere to the meninges
Angiostrongyliasis is an emerging food-borne infectious
or nerve root, causing missed diagnosis. Larvae of A. canto-
disease. The recent increase in angiostrongyliasis cases in
nensis were found in only 1.9% (56/3000) of patients with
China is thought to result from a geographic extension of
angiostrongyliasis.4 Therefore, the most commonly used tech-
the natural focus of A. cantonensis and changes in human
niques for diagnosing angiostrongyliasis are immunologic
dietary patterns. In this case, the patient was most likely in-
methods, including immunofluorescent antibody test,5 immu-
fected with A. cantonensis by ingestion of raw, parasitized
noenzyme staining test,6 and enzyme linked immunosorbent
snails (A. canaliculatus). Epidemiologic studies have impli-
assay.7 The antigens used in these methods are usually pre-
cated the African giant land snail, Achatina fulica,2 as the
pared from whole worm lysate. Although these tests are sen-
main snail vector for angiostrongyliasis in China. However,
sitive, they are not highly specific. Some researchers reported
golden apple snails (A. canaliculatus) also play an important
serological cross-reactivity between trichinosis and angio-
role because most cases of angiostrongyliasis documented in
strongyliasis.8 However, a 32-kd protein purified from young
the province of Guangdong are transmitted by this species.3
female worms of A. cantonensis is useful for detecting A.
This phenomenon could be explained by the fact that the
cantonensis infection with high sensitivity and specificity.9,10
local Cantonese seldom consume A. fulica. Furthermore,
The specific antigen and antibody of A. cantonensis in this
three of four A. canaliculatus collected from the same location
patient was identified by a method based on the 32-kd diag-
where the patient had obtained the snails he consumed were
infected with A. cantonensis, and the parasite load was high.
Patients with angiostrongyliasis often show brain abnor-
More than 6,000 A. cantonensis larvae were detected in a
malities. Tsai and others11 reported that most MRI findings in
single infective snail, and > 1,000 larvae were found in the
CNS infection with A. cantonensis are non-specific. Clinical
characteristics can range from normal to having leptomenin-
The detection rate for A. cantonensis is low because infec-
geal enhancement, ventriculomegaly, abnormal enhancement
tion occurs in the human central nervous system (CNS),
of punctate area, and hyperintense signal lesions on T2-
Fluid affenuated inversion recovery T2-weighted imaging of the brain. The arrows direct the high signal intensity that implies
multiple inflammatory foci in different areas.
weighted images. There seems to be a special predilection for
Feng Xu, Department of Neurological Internal Medicine, Wuyi Tra-
involvement of the globus pallidus and cerebral peduncle in
ditional Chinese Medical Hospital, Jiangmen, GD 529030, China.
some patients, and this correlates with the presence of wormsin the CSF, severity of headache, CSF pleocytosis, and eo-
sinophilia, as well as peripheral eosinophilia. The linear en-hancement of the spinal cord surface by contrast-enhanced
1. Chen XG, Li H, Lun ZR, 2005. Angiostrongyliasis, an emerging
T1WI spinal MRI also appears in cases of eosinophilic me-
food-borne infectious disease in mainland China. Emerg InfectDis 11: 1645–1647.
ningoencephalitis caused by infection of A. cantonensis.12 In
2. Wang QP, Chen XG, Lun ZR, 2007. Invasive freshwater snail,
this case, spot or patching enhancements on contrast-
China. Emerg Infect Dis 13: 1119–1120.
enhanced T2WI were observed in different areas of the brain.
3. Ding BL, He JZ, Zhu TC, Shen HX, 1984. Investigation on an-
There are different opinions of the proper treatment of
giostrongyliasis in Guangzhou area. Chin J Parasitol ParasticDis 2: 25–26. A. cantonensis infection. Some clinicians show that anthel-
4. Liang HK, 1988. The description of angiostrongyliasis. J Guang-
minthics, such as albendazole, ivermectin, mebendazole, and
pyrantel, do not provide clinical benefit, and many patients
5. Li XL, Chen XD, Lin XM, 1999. The detection of antibodies
have worsened while being treated with these therapies be-
against Angiostrongylus cantonensis with IFA. J Wenzhou Med
cause of the inflammatory reaction to antigens released by
6. Huang XQ, Zhong QC, He JZ, 1994. The detection of Angio-
dying worms.13 However, many studies in mainland China
strongylus cantonensis infection with IEST method. Chin J
have shown that anthelminthics can relieve symptoms and
shorten the course of disease. For example, Wang and oth-
7. Wang XT, Li FQ, Huang HJ, Li XY, 1999. Clinical significance of
ers14 reported that albendazole could relieve the symptoms of
the measurement of serum antibody against Angiostrongylus can-
angiostrongyliasis and suggested that it can be used to treat
tonensis by ELISA. Chin J Neuroimmunol Neurol 6: 128–130.
8. Maleewong W, Sombatsawat P, Intapan PM, Wongkham C,
the disease. Lin and others15 also reported that, in eight pa-
Chotmongkol V, 2001. Immunoblot evaluation of the specific-
tients who were treated with 20 mg/kg albendazole for 9 days,
ity of the 29 kDa antigen from young adult female worms
symptoms of acute angiostrongyliasis were rapidly relieved
Angiostrongylus cantonensis for immunodiagnosis of human
3–6 days after treatment. All of these patients recovered by 10
angiostrongyliasis. Asian Pac J Allergy Immunol 19: 267–273.
days after treatment, and no side effects were observed. In
9. Li H, Chen XG, Shen HX, Chen DX, Qiu YR, Hu XJ, 2005.
Value of the antigen with molecular mass of 32,000 in immu-
this case, the symptoms caused by the infection of A. canto-
nodiagnosis of Angiostrongylus cantonensis. J First Mil Mednensis were improved measurably after the treatment of al-
bendazole (20 mg/kg/d, for 7 days). Therefore, based on the
10. Li H, Chen XG, Shen HX, Peng HJ, Zhao XC, 2005. Antigen
documented reports and our experience, the use of anti-
analysis of Angiostrongylus cantonensis in different develop-
helminthics is recommended for the treatment of angio-
mental stages. Chin J Parasitol Parasit Dis 23: 36–39.
11. Tsai HC, Liu YC, Kunin CM, Lai PH, Lee SJ, Chen YS, Wann
strongyliasis, especially when infection is severe.
SR, Lin WR, Huang CK, Ger LP, Lin HH, Yen MY, 2003. Eosinophilic meningitis caused by Angiostrongylus cantonensis
Received March 30, 2008. Accepted for publication June 20, 2008.
associated with eating raw snails: correlation of brain magneticresonance imaging scans with clinical findings. Am J Trop Med
Acknowledgments: The authors thank Prof. Anthony A. James and
Dr. Jennifer Juhn for critical review of the manuscript and Yanping
12. Lai CH, Yen CM, Chin C, Chung HC, Kuo HC, Lin HH, 2007.
Chen for assistance in the analysis of MRI. The American Committee
Eosinophilic meningitis caused by Angiostrongylus cantonensis
on Clinical Tropical Medicine and Travelers’ Health (ACCTMTH)
after ingestion of raw frogs. Am J Trop Med Hyg 76: 399–402.
13. Pien FD, Pien BC, 1999. Angiostrongylus cantonensis eosinophil-
Financial support: This work was supported by a grant from the
ic meningitis. Int J Infect Dis 3: 161–163.
Ministry of Scientific and Technology of People’s Republic of China
14. Wang XT, Huang HJ, Dong QQ, Lin Y, Wang ZM, Li FQ, 1999.
A clinical research for eosinophilic meningoencephalitiscaused by angiostrongyliasis. Chin J Intern Med 38: 326–328.
Disclosure: The authors report no conflicts of interest.
15. Lin JX, Li YS, Zhu K, Chen BJ, Cheng YZ, Lin JC, Cao Y, Chen
Authors’ addresses: Hua Li, Jin-Bao Gu, and Xiao-Guang Chen, De-
RZ, 2003. Epidemiological study on group infection of Angio-
partment of Parasitology, School of Public Health and Tropical Medi-
strongylus cantonensis in Changle city. Chin J Parasitol Parasit
cine, Southern Medical University, Guangzhou GD 510515, China.
Curiosidades: Você sabia? Gripe suína A gripe suína refere-se à gripe causada pelas estirpes de vírus da gripe, chamadas vírus da gripe suína , que habitualmente infectam porcos, onde são endémicas. Em 2009 todas estas estirpes são encontradas no vírus da gripe C e nos subtipos do vírus da gripe A conhecidos como H1N1, H1N2, H3N1, H3N2, e H2N3. Quando os vírus
CONSENSUS STATEMENT THROMBOPHILIA AND VENOUS THROMBOEMBOLISM International Consensus Statement Guidelines According to Scientific Evidence The Cardiovascular Disease Educational and Research Trust, The International Union of Angiology and The Mediterranean League on Thromboembolism A. N. NICOLAIDES (Cyprus) (Chairman); H. K. BREDDIN (Germany); P. CARPENTIER (France);S. COCCHERI
 EOSINOPHILIC MENINGOENCEPHALITIS WITH A. CANTONENSIS
A, An A. canaliculatus (golden apple snail) collected from the place where the patient found the consumed snail. B, A third-stage
EOSINOPHILIC MENINGOENCEPHALITIS WITH A. CANTONENSIS
A, An A. canaliculatus (golden apple snail) collected from the place where the patient found the consumed snail. B, A third-stage