Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Neocontrol.de
Copyright 2005 by AMERICAN UROLOGICAL ASSOCIATION
DOI: 10.1097/01.ju.0000158445.68149.38
A PROSPECTIVE, RANDOMIZED, PLACEBO CONTROLLED, DOUBLE-
BLIND STUDY OF PELVIC ELECTROMAGNETIC THERAPY FOR THE
TREATMENT OF CHRONIC PELVIC PAIN SYNDROME WITH 1 YEAR OF
E. ROWE, C. SMITH, L. LAVERICK, J. ELKABIR, R. O’N WITHEROW AND A. PATEL
From the Department of Urology, St. Mary’s Hospital, London, United Kingdom
Purpose: Male chronic pelvic pain syndrome is a condition of uncertain etiology and treatment
is often unsatisfactory. There is evidence that the symptom complex may result from pelvic floormuscular dysfunction and/or neural hypersensitivity/inflammation. We hypothesized that theapplication of electromagnetic therapy may have a neuromodulating effect on pelvic floor spasmand neural hypersensitivity.
Materials and Methods: Following full Stamey localization men with National Institute of
Diabetes and Digestive and Kidney Diseases category III prostatitis were prospectively random-ized to receive active electromagnetic or placebo therapy. Active therapy consisted of 15 minutesof pelvic floor stimulation at a frequency of 10 Hz, followed by a further 15 minutes at 50 Hz,twice weekly for 4 weeks. Patients were evaluated at baseline, 3 months and 1 year aftertreatment using validated visual analog scores.
Results: A total of 21 men with a mean age of 47.8 years (range 25 to 67) were analyzed. Mean
symptom scores decreased significantly in the actively treated group at 3 months and 1 year(p Ͻ0.05), unlike the placebo group, which showed no significant change (p Ͼ0.05). Subanalysisof those receiving active treatment showed that the greatest improvement was in pain relatedsymptoms.
Conclusions: The novel use of pelvic floor electromagnetic therapy may be a promising new
noninvasive option for chronic pelvic pain syndrome in men.
KEY WORDS: pelvic pain, electromagnetics, prostate, pain, prostatitis
The uncertain etiology and variable response to treatment
cotherapy, particularly with regard to decreasing pain.9
has made prostatitis a challenging entity. In a national sur-
Therefore muscle tone in the urethra/sphincter mechanism
vey of physician visits in the United States a diagnosis of
may contribute to the pain experienced by men with CPPS.
prostatitis was made in 8% of urological and 1% of primary
Despite these findings the pathophysiology remains elusive
care physician visits, respectively.1 This confirmed it as a
and the role of neurogenic inflammation may offer a possible
significant health problem, supporting previous estimates of
explanation. It results from a complex interaction between the
approximately 2 million prostatitis related outpatient visits
central/peripheral nervous system and the immune system,
yearly nationwide.2 Globally the reported incidence of
causing the release of neuromediators that activate receptors
prostatitis-like symptoms has been shown to be 2.7% in the
on specific cells, including mast cells, Langerhans’ cells, micro-
Far East to 14.2% in Northern Europe.3, 4 In 1995 the Na-
vascular endothelial cells, fibroblasts and infiltrating immune
tional Institutes of Health-National Institute of Diabetes and
cells. The concept of neurogenic inflammation and its effect on
Digestive and Kidney Diseases (NIDDK) workshop reached a
mast cell function, vasoregulation and leukocyte recruitment in
consensus on the definition and classification of prostatitis
the pathophysiology of CPPS represents a new and interesting
syndromes.5 This has formed the basis for subsequent re-
avenue for further research.10, 11 Also, the role of purinergic
search on the pathophysiology of the disease and the efficacy
signaling through the release of urothelial adenosine triphos-
phate and the stimulation of subepithelial nerve plexus via the
The commonest and yet most poorly understood of these
purinergic P2X3 receptor, resulting in pain, may provide an
prostatitis syndromes is category III or chronic pelvic pain
explanation for the symptom profile seen in CPPS.12
syndrome (CPPS). It has been shown that, while men with
Conventional treatment has focused on long, empirical
CPPS have significantly higher leukocyte counts in urine and
courses of expensive broad-spectrum antibiotics, mostly of
expressed prostatic secretions compared with age matched
the quinolone class, with or without the concomitant use of
controls, inflammation and infection do not necessarily cor-
an ␣-blocker and anti-inflammatory agents. Stepwise intro-
relate with symptom severity.6, 7 The lack of a direct relation-
duction of these therapies has also been shown to be of
ship between inflammation and symptoms is supported
benefit.13 There is also emerging evidence of the benefits of
through studies of prostate histopathology, in which moder-
ate or severe inflammation was identified in only 5% of men
At the turn of the 19th century stimulation with electrical
current and changing magnetic fields was used to treat sur-
Contributory factors in the pathophysiology of CPPS may
face conditions associated with intractable pain, such as
include obstruction to bladder emptying. Symptomatic relief
painful malignant ulcers. The analgesic benefits of pulsed
has been demonstrated with the use of ␣-blocking pharma-
electromagnetic fields for relieving pelvic pain has been in-vestigated in women with tissue trauma and chronic refrac-
Submitted for publication July 19, 2004.
tory pelvic pain.15, 16 However, in the application of electro-
ELECTROMAGNETIC THERAPY FOR MALE CHRONIC PELVIC PAIN SYNDROME
magnetic stimulation to the pelvis most research has been inthe management of female stress and urge incontinence.
Despite its uncertain etiology there is some evidence that
the symptom complex found in CPPS may be founded at leastin part in pelvic floor muscular dysfunction and/or neuro-genic hypersensitivity/inflammation. We hypothesized thatthe application of a rapidly changing electromagnetic fieldapplied noninvasively to the perineum of the subject mayresult in neural excitation and pelvic floor muscle stimula-tion to a degree that breaks the cycle of tonic muscular spasmand neural hypersensitivity/inflammation, thereby, restoringmore normal pelvic floor muscular activity.
A total of 21 men attending the urology outpatient clinic
with a diagnosis of NIDDK category IIIA or IIIB prostatitissyndrome were invited to take part in a trial of electromag-netic pelvic floor therapy. Entry criteria were age 70 years orless and a full Stamey procedure to exclude urinary microor-ganisms. Prostate cancer had been excluded by normal se-rum prostate specific antigen, clinically benign digital rectalexamination or negative previous biopsy. Patients with pre-vious pelvic radiotherapy were also excluded.
Each man had previously undergone several types of failed
medical therapy for the condition, which typically included
FIG. 1. Neotonus™ electromagnetic chair. Reproduced with per-
multiple antibiotic courses, ␣-blockers and occasionally anti-
depressants. After obtaining informed consent eligible sub-jects were randomized to active and placebo groups usingcomputer generated, blocked randomization numbers. Pa-
tients were informed about the nature of the treatment, the
A total of 21 men with a mean age of 47.8 years (range 25
treatment schedule and the possibility that they might be
to 67) were entered into the study. Of the 21 men 11 were
randomized to placebo but they were not given a detailed
randomized to the active treatment group and 10 were ran-
description of what local pelvic sensations, if any, to expect
domized to the placebo treatment group. Four men failed to
during treatment, so as not to bias blinding.
complete the 4-week treatment, including 1 in the active
All men were asked to complete a baseline symptom visual
treatment group and 3 in the placebo group. They were
analog score (VAS) questionnaire that included 5 items of
excluded from further analysis. Followup data were obtained
pain related questions and 4 covering urinary symptoms (see
on 17 men at 3 months (10 in the active and 7 in the placebo
Appendix). The VAS questionnaire was adopted from the
group) and 13 at 1 year (8 and 5, respectively).
validated symptom severity index designed by Nickel and
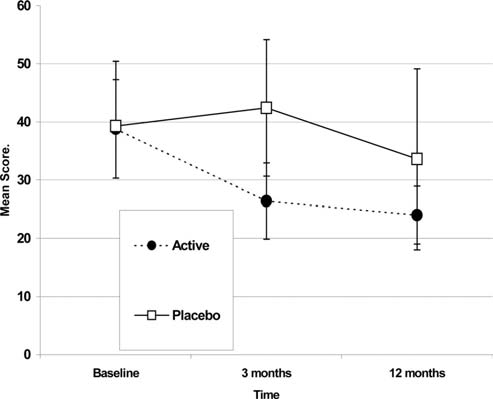
A significant difference was observed when mean symptom
Sorensen.17 The question regarding painful digital rectal ex-
scores in the active and placebo groups were analyzed. There
amination was omitted because the questionnaire was
was a statistically significant decrease in mean symptom scores
mailed and, hence, clinical evaluation was not possible. Each
in the active treatment arm from 38.8 of 90 at baseline to 26.4
individual question was scored from 0 —asymptomatic to
of 90 at 3 months (95% CI 0.9 to 21.9, p Ͻ0.05) and to 24.0 of 90
10 —severely symptomatic, providing a total score of 0 to 90.
at 1 year (95% CI 0.15 to 30.85, p Ͻ0.05). There was no statis-
The symptom score questionnaire was re-administered 3
tically significant change in symptom scores in the placebo
months and again 1 year following treatment in a double-
group, which remained relatively unchanged at mean of 39.3
blind manner with patients and the individual analyzing the
of 90 at baseline, 42.4 of 90 at 3 months (95% CI Ϫ1.7 to 22.37,
data blinded to the identity of those who had received active
p Ͼ0.05) and 33.6 of 90 at 1 year (95% CI Ϫ32.66 to 28.26,
The active treatment regime was empirical and consisted
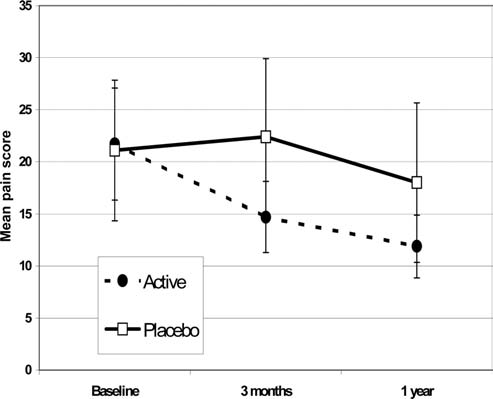
On differential analysis separating pain scores from urina-
of 2 sessions weekly for 4 weeks (total 8 sessions). During
tion scores similar improvement was seen in the active treat-ment group. The pain score decreased significantly in those
each half-hour session the patient would sit centrally on the
receiving active treatment from a mean baseline of 21.7 of 50
Neotonus™ electromagnetic chair for 2 consecutive 15-
to 14.7 of 50 at 3 months (95% CI 3.57 to 12.43, p Ͻ0.05) and
minute periods (fig. 1). The frequency was set low at 10 Hz for
to 11.9 of 50 at 1 year (95% CI 2.8 to 18.7, p Ͻ0.05). The mean
the first 15-minute period and increased to 50 Hz for the
pain score in the placebo group remained relatively un-
second 15-minute period. The gain was set low initially and
changed for the same periods, that is 21.1 of 50 at baseline,
gradually increased, as tolerated by the patient. Patients
22.4 of 50 at 3 months (95% CI Ϫ16.38 to 13.8, p Ͼ0.05) and
who received placebo were treated in a manner identical to
18 of 50 at 1 year (95% CI Ϫ22.6 to 19.8, p Ͼ0.05, fig. 3).
that in the active treatment group in all respects except no
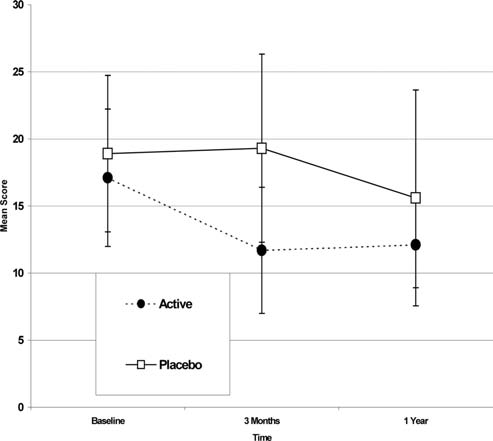
Mean urinary symptom scores showed a significant de-
active stimulation was applied from the device. Instead, the
crease from 17.1 of 40 at baseline to 11.7 of 40 at 3 months in
chair was switched on so that the fan could be heard and a
those receiving active treatment (95% CI 1.2 to 12.4,
hidden speaker under the stimulation device replicated the
p Ͻ0.05). While mean urinary symptom scores remained
sounds created during active treatment. Men receiving active
below baseline at the 1-year followup, improvement in the
and placebo therapy were treated on alternate days to pre-
actively treated group no longer achieved statistical signifi-
vent cross-talk between groups, which may have compro-
cance. There was no corresponding improvement in urinary
mised study blinding. Statistical analysis was performed us-
symptoms in the placebo group, which changed little from the
baseline of 18.9 of 40 to 19.3 of 40 at 3 months (95% CI Ϫ6.5
ELECTROMAGNETIC THERAPY FOR MALE CHRONIC PELVIC PAIN SYNDROME
FIG. 2. Mean VAS pain and urinary symptom scores at baseline,
and 3 and 12 months in active and placebo groups.
FIG. 4. Mean urinary symptom scores in active and placebo
categories of men receiving active treatment, which was sus-tained at 1 year. There was also a significant improvement inurinary symptoms at 3 months of followup in the activegroup, although this decrease was of lower magnitude thanthe improvement in pain symptoms (approximately 30%) andit was no longer significantly different from baseline at 1year. Nevertheless, no equivalent improvement was seen inthe placebo group. Although we did not test the effectivenessof blinding the sham treatment group, we believe that thedifferences that we observed represent a real effect throughmechanisms that have yet to be elucidated. Since this was apilot study, quantitative analysis of the effectiveness of blind-ing to active or placebo treatment was not done and thisshould be part of any future study. However, because men ineach arm wrote to ask if they had received active treatmentat the 1-year followup, this anecdotal evidence reassured usas to the effectiveness of blinding. The failure to obtain fol-lowup data on all of those who participated in the study is atleast in part a reflection of the transient nature of the urban
FIG. 3. Mean pain scores at baseline, and at 3-month and 1-year
population in which this study was performed.
While the precise etiology of CPPS continues to be obscure,
there is growing evidence that it may result from muscular/neural dysfunction of the lower urinary tract rather from
to 5.64, p Ͼ0.05) and 15.6 of 40 at 1 year (95% CI Ϫ11.83 to
than an inflammatory process in the prostate gland, which is
supported by histological evidence and the failure of antibi-
No significant side effects were observed. One patient in
otic treatment in a randomized, placebo controlled, multi-
the active group experienced transient paresthesia 48 hours
center trial.8, 18 Support for the theory that it may result from
in duration with subsequent complete resolution.
a spasm in the proximal sphincter mechanism may derivefrom the decrease in symptoms in men treated with
␣-blockers.13,19 However, the pathways in neurogenic in-
In this pilot study we prospectively tested the hypothesis
flammation and in particular the complex interaction be-
that pelvic floor neuromuscular dysfunction/neurogenic in-
tween central and peripheral nervous and the endocrine sys-
flammation may account for some symptoms of CPPS
tem, and their effects on immunomodulatory mechanisms
(NIDDK IIIA and IIIB) and this dysfunction could be de-
may provide an explanation for the symptom pattern seen in
creased by the noninvasive application of local electromag-
men with CPPS. The modification/interruption of this path-
netic therapy. Sustained improvement was observed in the
way through electromagnetic stimulation may explain the
symptom scores of men in the active group compared with
improved symptom profile in those who received active treat-
scores those who received sham treatment.
ment. By breaking the cycle of tonic muscular spasm and
When mean symptom scores were compared at 3 months
neural hypersensitivity/inflammation normal pelvic floor
and 1 year, there was a statistically significant decrease of
muscular activity is restored. This may account for the du-
approximately 40% in men in the active group, which was not
rability of the response. Another possible explanation is that
observed in the placebo group. Further subanalysis of VAS
purinergic P2X3 receptor subunits are up-regulated in CPPS,
pain and urinary symptom scores showed that the greatest
as reported in interstitial cystitis, and this up-regulation is
improvement in the symptom profile was seen in the pain
reversed or there is desensitization of purinergic receptors
ELECTROMAGNETIC THERAPY FOR MALE CHRONIC PELVIC PAIN SYNDROME
following treatment.12 Interference of this pathway could
2. Long-Range Plan Window on the 21st Century. National Kidney
explain why pain symptoms showed the greatest response.
and Urologic Diseases Advisory Board. Bethesda, Maryland:
To date electromagnetic stimulation therapy has generally
United States Department of Health and Human Services,
been reserved for stress and urge female urinary inconti-
National Institutes of Health Publication No. 90 –583, p. 20,
nence. The frequencies used for this purpose were 10 and 50
Hz. Hence, these frequencies were applied in our phase II
3. Tan, J. K., Png, D. J., Liew, L. C., Li, M. K. and Wong, M. L.:
study. It may be that a single frequency will suffice and
Prevalence of prostatitis-like symptoms in Singapore: a
shorten treatment time, leading to cost savings. Frequencies
population-based study. Singapore Med J, 43: 189, 2002
of 20 Hz have been used successfully in the treatment of
4. Mehik, A., Hellstrom, P., Lukkarinen, O., Sarpola, A. and
detrusor hyperreflexia, showing functional responses in the
Jarvelin, M.: Epidemiology of prostatitis in Finnish men: a population-based cross-sectional study. BJU Int, 86: 443, 2000
pelvic sphincter muscles together with an inhibition of de-
5. National Institutes of Health-National Institute of Diabetes and
trusor hyperreflexia, possibly via the activation of pudendal
Digestive and Kidney Diseases Workshop on Chronic Prostati-
nerve afferents blocking parasympathetic detrusor motor fi-
tis: Summary Statement. Bethesda, Maryland: United States
bers at the spinal reflex arc.20 If the changing electromag-
Department of Health and Human Services, 1995
netic field exerts its effect in CPPS by decreasing tone in the
6. Nickel, J. C., Alexander, R. B., Schaeffer, A. J., Landis, J. R.,
proximal sphincter mechanism, frequencies with a maximal
Knauss, J. S., Propert, K. J. et al: Leukocytes and bacteria in
effect at this site may prove more effective.
men with chronic prostatitis/chronic pelvic pain syndrome
The electromagnetic chair is unlikely to exert its effect on
compared to asymptomatic controls. J Urol, 170: 818, 2003
pain pathways similar to a transcutaneous electrical nerve
7. Schaeffer, A. J., Knauss, J. S., Landis, J. R., Propert, K. J.,
stimulation machine. 1) This would not account for the im-
Alexander, R. B., Litwin, M. S. et al: Leukocyte and bacterial
provement in urinary symptoms. 2) The transcutaneous elec-
counts do not correlate with severity of symptoms in men with
trical nerve stimulation machine operates at a much higher
chronic prostatitis: the National Institutes of Health Chronic
frequency of 120 Hz. The noninvasive nature of electromag-
Prostatitis Cohort Study. J Urol, 168: 1048, 2002
netic stimulation treatment and the ease of repeating it if
8. True, L. D., Berger, R. E., Rothman, I., Ross, S. O. and Krieger,
necessary makes it attractive to patients and physicians
J. N.: Prostate histopathology and the chronic prostatitis/
alike since it can be easily performed in the office environ-
chronic pelvic pain syndrome: a prospective biopsy study.
J Urol, 162: 2014, 1999
9. Mehik, A., Alas, P., Nickel, J. C., Sarpola, A. and Helstrom, P. J.:
Alfuzosin treatment for chronic prostatitis/chronic pelvic pain
In this study we noted the safe, effective and novel use of a
syndrome: a prospective, randomized, double-blind, placebo- controlled, pilot study. Urology, 62: 425, 2003
noninvasive pelvic floor stimulation device, that is the elec-
10. Mehik, A., Leskinen, M. J. and Hellstrom, P.: Mechanisms of
tromagnetic chair, for treating CPPS symptoms in a prospec-
pain in chronic pelvic pain syndrome: influence of prostatic
tive, double-blind, placebo controlled study. These subjective
inflammation. World J Urol, 21: 90, 2003
improvements at 3 months of followup in patients in whom
11. Wesselmann, U.: Neurogenic inflammation and chronic pelvic
many other treatment regimens have previously failed were
pain. World J Urol, 19: 180, 2001
durable in the majority at 1 year. Further large-scale multi-
12. Sun, Y. and Chai, T. C.: Up-regulation of P2X receptor during
center studies are required fully to evaluate the efficacy of
stretch of bladder urothelial cells from patients with intersti-
this treatment and establish the optimal stimulation fre-
tial cystitis. J Urol, 171: 448, 2004
quency as well as the usefulness of repeating treatment in
13. Shoskes, D. A., Hakim, L., Ghoniem, G. and Jackson, C. L.:
those in whom initial therapy fails. These studies should
Long-term results of multimodal therapy for chronic prostati-
incorporate the National Institute of Health CPPS index as a
tis/chronic pelvic pain syndrome. J Urol, 169: 1406, 2003
primary outcome measure, which was unfortunately not pub-
14. Kaplan, S. A., Volpe, M. A. and Te, A. E.: A prospective, 1-year
lished at the time of initiation of this study.
trial using saw palmetto versus finasteride in the treatment ofcategory III prostatitis/chronic pelvic pain syndrome. J Urol,
Robert Redfern assisted with statistical data analysis. 171: 284, 2004
Neotonus™ provided the electromagnetic chair.
15. Jorgensen, W. A., Frome, B. M. and Wallach, C.: Electrochemical
therapy of pelvic pain: effects of pulsed electromagnetic fields
(PEMF) on tissue trauma. Eur J Surg Suppl, 574: 83, 1994
Each symptom category was scored from 0 (asymptomatic)
16. Varcaccio-Garofalo, G., Carriero, C., Loizzo, M. R., Amoruso, S.
and Loizzi, P.: Analgesic properties of electromagnetic field
1) Pain or discomfort in the penis, testicles or scrotum
therapy in patients with chronic pelvic pain. Clin Exp Obstet
2) Pain or discomfort in the perineum (area where you sit,
Gynecol, 22: 350, 1995
17. Nickel, J. C. and Sorensen, R.: Transurethral microwave ther-
3) Pain or discomfort in the suprapubic or bladder area
motherapy for nonbacterial prostatitis: a randomized double-
blind sham controlled study using new prostatitis specific as- sessment questionnaires. J Urol, 155: 1950, 1996
5) Pain or discomfort in the low back, upper leg or groin
18. Nickel, J. C., Downey, J., Clark, J., Casey, R. W., Pommerville,
P. J., Barkin, J. et al: Levofloxacin for chronic prostatitis/
6) Uncomfortable and difficult urination (stranguria)
chronic pelvic pain syndrome in men: a randomized placebo-
controlled multicenter trial. Urology, 62: 614, 2003
8) Difficulty postponing urination (urgency)
19. Barbalias, G. A., Nikiforidis, G. and Liatsikos, E. N.: ␣-Blockers
9) Burning feeling during urination (dysuria)
for the treatment of chronic prostatitis in combination with antibiotics. J Urol, 159: 883, 1998
20. Sheriff, M. K., Shah, P. J., Fowler, C., Mundy, A. R. and Craggs,
1. Collins, M. M., Stafford, R. S., O’Leary, M. P. and Barry, M. J.:
M. D.: Neuromodulation of detrusor hyper-reflexia by func-
How common is prostatitis? A national survey of physician
tional magnetic stimulation of the sacral roots. Br J Urol, 78:
visits. J Urol, 159: 1224, 1998
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use ----------------------------- ADVERSE REACTIONS -------------------------------------- GRALISE safely and effectively. See full prescribing information for The most common adverse reaction (greater than or equal to 5% and twice GRALISE. GRALISE® (gabapentin) tablets I
Rosenberg Gesellschaft für ganzheitliche Gesundheit & Bildung gemeinnützige GmbH Mit Ayurveda fit durch den Winter Artikel von Kerstin Rosenberg Auch vor dem heute vorherrschenden Klimachaos und global warming warnten die alten, ayurvedi-schen Schriften bereits vor den Gefahren, denen sich unser Körper zu den wechselnden Jahreszeitenausgesetzt. Denn entsprechend der untersc
 Copyright 2005 by AMERICAN UROLOGICAL ASSOCIATION
DOI: 10.1097/01.ju.0000158445.68149.38
Copyright 2005 by AMERICAN UROLOGICAL ASSOCIATION
DOI: 10.1097/01.ju.0000158445.68149.38
 ELECTROMAGNETIC THERAPY FOR MALE CHRONIC PELVIC PAIN SYNDROME
magnetic stimulation to the pelvis most research has been inthe management of female stress and urge incontinence.
ELECTROMAGNETIC THERAPY FOR MALE CHRONIC PELVIC PAIN SYNDROME
magnetic stimulation to the pelvis most research has been inthe management of female stress and urge incontinence.
 ELECTROMAGNETIC THERAPY FOR MALE CHRONIC PELVIC PAIN SYNDROME
FIG. 2. Mean VAS pain and urinary symptom scores at baseline,
and 3 and 12 months in active and placebo groups.
ELECTROMAGNETIC THERAPY FOR MALE CHRONIC PELVIC PAIN SYNDROME
FIG. 2. Mean VAS pain and urinary symptom scores at baseline,
and 3 and 12 months in active and placebo groups. ELECTROMAGNETIC THERAPY FOR MALE CHRONIC PELVIC PAIN SYNDROME
following treatment.12 Interference of this pathway could
2. Long-Range Plan Window on the 21st Century. National Kidney
explain why pain symptoms showed the greatest response.
ELECTROMAGNETIC THERAPY FOR MALE CHRONIC PELVIC PAIN SYNDROME
following treatment.12 Interference of this pathway could
2. Long-Range Plan Window on the 21st Century. National Kidney
explain why pain symptoms showed the greatest response.