Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Microsoft word - npquestion.docx
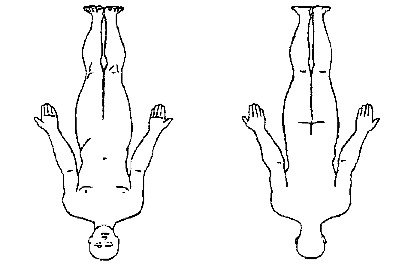
PAIN SOLUTIONS NEW PATIENT QUESTIONNAIRE Patient Name: __________________ DATE______________________ Primary Doctor: _____________________________ Referring Doctor: _____________________ Please show the location of your pain by drawing on the figures below:
Pain History (PLEASE FILL IN THE BUBBLES)
1. WHERE IS YOUR PAIN LOCATED?
2. WHERE DOES THE PAIN RADIATE? 3. THE PAIN FIRST STARTED: Was there an accident or injury that caused the pain?
O YES _____________________________________________________________________
4. HOW WOULD YOU DESCRIBE YOUR PAIN? (mark all that apply)
5. RATE YOUR PAIN AT IT’S WORST IN THE LAST 24 HOURS?
6. RATE YOUR PAIN AT IT’S BEST IN THE LAST 24 HOURS?
7. HOW SEVERE IS YOUR PAIN ON AVERAGE?
8. HOW MUCH DOES THE PAIN INTERFERE WITH YOUR ACTIVITIES?
9. HOW MUCH DOES THE PAIN INTERFERE WITH YOUR SLEEP?
10. THE PAIN IS:
11. WHAT MAKES THE PAIN WORSE?
12. WHAT MAKES THE PAIN BETTER?
13. IN ADDITION TO THE PAIN, DO YOU HAVE?
14. IS YOUR PAIN:
15. WHAT TESTS HAVE YOU HAD FOR YOUR PAIN? (Please list date of last exam)
O MRI Scan_____________ O CT Scan____________
16. WHAT MEDICATIONS HAVE YOU TRIED FOR YOUR PAIN? (Check ALL that apply) Anti-Inflammatory: O Ibuprofen (Advil, Motrin) Narcotic: Antidepressants
O Fluoxetine (Prozac) O Escitalopram (Lexapro)
O Venflaxine (Effexor) O Sertraline (Zoloft)
O Nortriptyline (Pamelor) O Desipramine (Norpramine)
O Citalopram (Celexa) O Paroxetine (Paxil)
Anti-Seizure
O Pregabalin (Lyrica) O Zonisamide (Zonegram)
O Lamotrigine (Lamictal) O Oxycarbazepine (Trileptal)
Muscle Relaxants/
O Tizanidine (Zanaflex) O Metaxolone (Skelaxin)
Anti-Anxiety
O Cyclobenzaprine (Flexeril) O Methocarbamol (Robaxin)
Sleeping Aids Other Pain Meds
17. WHAT TREATMENTS HAVE YOU HAD FOR YOUR PAIN?
O Other __________________________________________________
Past Medical History (Please Fill in “yes” or “no” to all questions) CARDIOVASCULAR GASTOINTESTINAL RESPIRATORY NEUROLOGY
Social History
Drug(s) Used ____________________________________
OTHER SYMPTOMS (Please indicate other symptoms you may have) CONSTITUTIONAL NEUROLOGY RESPIRATORY MUSCULOSKELETAL CARDIOVASCULAR HEMATOLOGY CURRENT MEDICATIONS (Include dosage and # tablets per day)
Have you had any surgeries? _____________________________________________________ ______________________________________________________________________________ ______________________________________________________________________________ Are you taking any of the following blood thinners? ___ Coumadin ___ Plavix Do you have any allergies to medications? ___ Latex ___ Iodine __Other Medications? ___________________
What are your goals for your pain treatment? __________________________________________________________________________________ __________________________________________________________________________________ Are there any specific treatments that you would like for your pain? Medications: __________________________________________________ Physical Therapy: ______________________________________________ Exercise: ______________________________________________________ Psychologist referral: ___________________________________________ Surgery referral ________________________________________________ Injections: ______________________________________________________ Other pain therapies: (Please circle) Do you have a driver with you today? __ yes __ no THIS IS THE END OF THE QUESTIONNAIRE. THANK YOU!
The 2nd International Congress of Large Animal PractitionersClinical signs and oocyst shedding pattern in cryptosporidiosis and its correlation with retarded growth and weight loss in neonatal calves Low levels of Clostridium perfingense toxins as a probable predisposing factor for septicemic Pasteurella multocida infection in sheep Pregnancy toxemia following oral antibiotic administration
Fit Measurement: How to Distinguish Between Fit and Notes for Brainstorming Session prepared by Pnina Soffer Discussion mission 1. To characterize approaches to fit assessment and identification. 2. To characterize fit maintenance triggers and policies, and factors that should Motivation Business processes may change frequently, as the business environment is dynamic and constantly e
 PAIN SOLUTIONS
PAIN SOLUTIONS