Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Microsoft word - manuscript 081003 c.doc
Reduced hospital stay, morphine consumption, and pain intensity with local infiltration analgesia after unicompartmental knee arthroplasty. A randomized double-blind study of 40 patients
Per Essving1, Kjell Axelsson2, Jill Kjellberg2, Örjan Wallgren1, Anil Gupta2,
___________________________________________________________________________
1Department of Orthopedic Surgery and 2Department of Anesthesiology and Intensive Care,
Institution for Clinical Medicine, University Hospital, Örebro, Sweden
Correspondence PE: per.essving@orebroll.se
Background and purpose: Postoperative pain is moderate-severe following knee arthroplasty.
We investigated the efficacy of local administration of analgesics into the operating field,
Methods: 40 patients undergoing uni-compartmental knee arthroplasty (UKA) were
randomized in a double-blind study into two groups (Clinical Trials.gov NCT00653926). In
group A (Active), 200 mg ropivacaine, 30 mg ketorolac and 0.5 mg epinephrine (total volume
106 mL) were infiltrated intra-operatively into the soft tissue, while in group P (Placebo), no
injections were given. At 21 postoperative hours, 150 mg ropivacain, 30 mg ketorolac and 0.1
mg epinephrine were injected intraarticularly via a catheter in group A, and the same volume
(22ml) of saline was injected in group P.
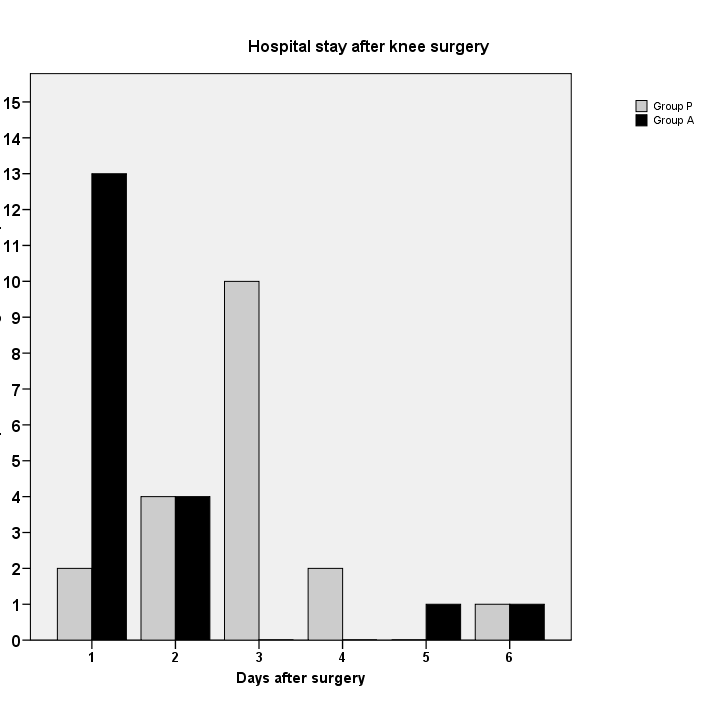
Results: Median Hospital stay was shorter in group A compared to group P: 1 (1-6) vs. 3 (1-
6) days (p < 0.001). Postoperative pain in group A was significantly lower at rest after 6 h and
27 h and on movement after 6, 12, 22 and 27 h. Morphine consumption were significantly
lower in group A during 0-48 h, resulting in lower frequency of nausea, pruritus and sedation.
Improved functional scores were found within both groups by Oxford Knee Score and EQ-5D
postoperatively compared to preoperative values.
Interpretation: Local injection of analgesics periarticularly at the end of the operation and
intraarticularly after 21 h postoperatively provided excellent pain relief and earlier home
discharge following UKA. High satisfaction was found in both groups after 6 months.
Introduction
Postoperative pain is often severe following knee arthroplasty (Wang et al. 2002).
Traditionally, this has been managed by epidural analgesia, continuous peripheral nerve
blocks or parental opioid drugs. Although epidural analgesia is efficacious (Axelsson et al.
2005), side effects and some rare but major complications such as spinal hemorrhage and
spinal infection have recently questioned its routine use, specifically in older women (Moen et
al. 2004). Peripheral nerve blocks provide good analgesia, but in order to effectively control
pain, it may be necessary to block the sciatic, femoral and obturator nerves (McNamee et al.
2002), which can be technically demanding. Parental opioids are associated with side effects.
This has lead to a search for new strategies, to avoid the problems of regional analgesia or
opioids, and to minimise the complications.
Recently, a local infiltration analgesia (LIA) technique was developed by Drs Kerr and Kohan
in Sydney, Australia(Rostlund and Kehlet 2007, Kerr and Kohan 2008). With this LIA-
technique, a long-acting local anesthetic (ropivacaine), a nonsteroidal anti-inflammatory drug
(ketorolac), and epinephrine are infiltrated periarticularly intraoperatively and via an
intraarticular catheter postoperatively. Effective pain relief with early mobilization and
Minimal invasive techniques for arthroplasty have become increasingly popular, especially
for unicompartmental knee arthroplasty (UKA) in medial non-inflammatory arthritis.
Together with an intraoperative multimodal analgesia program and rapid mobilization, the
minimal invasive technique is believed to further decrease the hospital stay (Beard et al. 2002,
Reilly et al. 2005, Carlsson et al. 2006, Berend and Lombardi 2007). However, the specific
role of the LIA-technique has not been fully investigated in double-blind studies.
The primary aim of this double-blind study was to evaluate if intra- and postoperative
administration of ropivacaine, ketorolac and epinephrine into the operating field would affect
the length of hospital stay. Secondary end-points were morphine consumption, pain intensity
and side effects. In an attempt to assess the safety of this technique, knee function and patient
satisfaction scores were also assessed for up to 6 months after surgery.
Patients and methods
The study protocol was approved by the regional ethics committee (May 4, 2005, EudraCt nr
no. 2005-000685-39) and the Swedish Medical Products Agency and conducted in accordance
with the Declaration of Helsinki (Clinical Trials.gov Identifier: NCT00653926).
57 consecutive patients scheduled for unicompartmental knee arthroplasty (UKA) because of
osteoarthritis, were screened for eligibility. The inclusion criteria were: age 20-80 years, ASA
physical status I-III and mobility indicating normal preoperative mobilization. Exclusion
criteria included known allergy or intolerance to one of the study drugs, serious liver-, heart-
or renal decease, chronic pain or bleeding disorder.
Randomization and blinding
57 patients were assessed for eligibility and 17 were excluded prior to randomization; see
flow chart for details (Figure 1). Therefore, 40 patients were enrolled in this randomized
double-blind study. Written informed consent was obtained from each patient before the start
of the study. Surgery was performed at the Department of Orthopaedics, Örebro University
Hospital during September 2005 and March 2007 and patients were followed for 6 months
The Hospital Pharmacy randomized the patients into 2 groups, 20 patients in each, using
computer-generated randomized numbers. Group A (Active) received a multimodal injection
intra- and postoperatively while group P (Placebo) received no injection intraoperatively and
a saline injection postoperatively as described in details below. On the day before or on the
morning of surgery, the surgeon called the Hospital Pharmacy to receive the group
randomization. The patients, the two study investigators, the study physiotherapist and all the
staff concerned with the postoperative care of the patients were blinded. Since the operating
surgeons were not blinded, they did not take part in the patient care after completion of the
Anesthesia
All patients received diazepam 10 mg orally 1 hour before planned surgery and all operations
were performed under general anesthesia. When designing this study, we decided not to use
spinal or epidural anesthesia in order to be able to assess differences in early postoperative
pain and mobilization more accurately, and to ensure blinding of the patients to the treatment
group. Cloxacillin 1 g was given intravenously before surgery and at 8, 16 and 24 h
postoperatively. Dalteparin 5000 IU was administered subcutaneously once each evening for
10 days, starting on the evening before surgery, for thrombo-prophylaxis.
Surgery
All operations were performed by using a minimally invasive technique. The same technique
was used in both groups and all patients received the Link Endo-Model Sled Prosthesis (Link
Sweden AB, Akersberga, Sweden). A tourniquet was used in all patients.
Pain management
In group A, 200 mg ropivicaine, 30 mg ketorolac and 0.5 mg epinephrine (total volume 106
mL) were infiltrated by the surgeon into the soft tissues peri-articularly during the operation
in the following way: Before inserting the components, 20-30 mL were injected into the
posterior capsule and before closure of the wound, the rest was injected into the capsule
incision, the synovium, the ligament and the subcutaneous tissue. In group P no injections
were given. All patients had a tunnelled intraarticular multihole 20-G catheter placed at the
end of the operation by the surgeon. No drain was placed in the wound. A compression
bandage and ice packs were applied during the first 6 hours. A Patient Controlled Analgesia
(PCA)-pump with morphine (1-mg bolus with 6-min lockout time) was connected IV, which
was used as rescue medication by all patients. All patients received 1 g paracetamol orally 4
times a day, starting the preoperative morning. After 21 hours, 150 mg ropivicaine, 30 mg
ketorolac and 0.1 mg epinephrine, total volume 22 mL, were injected intraarticularly via the
catheter in group A and a similar volume of saline was injected in group P. Pain assessments
were made by using a 100-mm Visual Analogue Scale (VAS) and, at 24 h, if pain at rest was
< 40 on the VAS during a 2 h period, the PCA-pump was discontinued and paracetamol 1 g
and tramadol 50 mg orally were administered up to 4 times daily as needed. The intraarticular
catheter was removed after 24 h and the tip of the catheter was sent for culture.
Mobilization and home discharge
The first attempt to mobilization was made 6 h postoperatively when the patient was
encouraged to stand up and to walk 2-3 steps. If unsuccessful, mobilization was attempted
again on the following day. The patients were discharged when they fulfilled the discharge
criteria (see below). After discharge, the patients were asked to complete a questionnaire
regarding postoperative pain on days 1, 3 and 14.
Outcome measures
Hospital stay: The time to home discharge (day 0 = the day of operation) was assessed by a
physician and the study physiotherapist who was unaware of the group randomization
according to the following criteria: mild pain (VAS < 30) sufficiently controlled by oral
analgesics, able to walk with elbow crutches, ability to climb 8 stairs, eat and drink, and no
Pain: Pain assessment (VAS) were made at 3, 6, 12, 21, 22 (i.e. 1 h after test drug injection in
knee catheter), 27 hours, on day 3, 14 and at 3 and 6 months postoperatively. Pain was
assessed both at rest and on motion (60 degrees of knee flexion).
Analgesic consumption: Morphine consumption was recorded during 0–6, 0–24 and 24–48
hours postoperatively. Oral analgesic consumption was recorded during 0-24, 24-48, 48-96
Surgical outcomes: The physiotherapist recorded the ability to walk with a walking frame 6
hours postoperatively. Knee extension and flexion were assessed preoperatively, at 27 hours,
at discharge, on day 3, and at 3 and 6 months postoperatively. Patient satisfaction during the
first 24 postoperative hours and after 7 days was rated. Oxford Knee Score was determined
preoperatively, and at 2 weeks, 3 and 6 months postoperatively. Oxford Knee Score is a
validated 12-item knee questionnaire that scores patients from 12 (the best possible) to 60 (the
worst possible) (Jahromi et al. 2004). EuroCol (EQ-5D) questionnaire was collected
preoperatively, and postoperatively at 6 months. EuroCol (EQ-5D) is a standardized
instrument for use as a measure of health outcome (Fransen and Edmonds 1999). It provides a
single index value from 0 to 1 where 0 represents poor health and 1 represents perfect health.
All complications and adverse events were registered intra- and postoperatively as well as
after discharge. Hospital readmission during the 6 months follow-up period postoperatively
Statistics
A power analysis was done prior to the start of the study using length of hospital stay (LOS)
as the primary end-point. In a pilot study on 8 patients, the LOS for the intervention group
was found to be 3.1 (SD 1.3). In a similar group of patients, operated earlier without the LIA-
technique, the mean LOS was 5.5 (SD 1.5) days. With a α = 0.05 and a β = 0.2 and expected
reduction of 1.5 days in the treatment group and a standard deviation of 1.5, 17 patients would
be required in each group. Assuming a somewhat greater standard deviation in the control
group, 20 patients were included in each group in the study.
The Mann-Whitney-U test was used for the analysis of the primary end-point (LOS) since the
data were not found to be normally distributed. Results are presented as median and 95% CI.
The VAS was assessed as a supportive parameter and analysed as if it was a primary
endpoint. Mann-Whitney-U test was used to assess median pain scores and the p-values were
corrected using the Bonferroni-Holm method. The other secondary end-points (morphine
consumption, knee function scores and patient satisfaction scores) were also analysed using
the Mann-Whitney-U test. Dichotomous data was analyzed using the chi-square test or
Fisher’s exact test, as appropriate. A value of p < 0.05 was considered to be statistically
Patients
Two patients of the 40 patients enrolled in the study were excluded, 1 in group A due to
catheter disconnection and 1 in group P due to intra-operative conversion to total knee
arthroplasty, thus 38 patients completed the study. Patient characteristics were similar in both
Primary end-point: Hospital stay
Analysis of results when including all 40 patients (intention-to-treat principle) or 38 patients
(per-protocol principle) did not reveal any statistically significant differences. The
postoperative hospital stay was shorter in group A (n = 19) than in group P (n = 19), median
(range) values 1(1-6) vs. 3(1-6) days (p < 0.001), i.e. a difference of 2 (CI 95% 1 – 2) days
(Figure 2). In group A 13/19 patients were discharged during the first postoperative day
compared to 2/19 in Group P (p < 0.001). During the first 2 postoperative days 17/19 vs. 6/19
patients were discharged in group A compared to group P (p < 0.001).
5 patients (2 patients in group A and 3 patients in group P) had prolonged hospital stay due to
pain and were discharged after the third postoperative day.
Secondary end-points: Pain relief
At rest (Figure 3), VAS pain score was lower in group A than in group P at 6 h (p=0.003) and
27 h (p=0.004). At 6 months only 3 patients had registered pain in group A (5, 6, 21 mm)
whereas in group P, all patients had VAS 0 mm.
On movement (Figure 4), VAS pain score were significantly lower in Group A compared to
Group P at 6, 12 and 22 hours (all with p<0.001) and 27 h (p=0.001). At 6 months all patients
Analgesic consumption
Median (range) morphine consumption was lower in group A than in group P: 21 (0-68) mg
vs. 67 (17-126) mg during 0-48 h postoperatively (p < 0.001). During 24-48 h there were only
2 patients in group A compared to12 patients in group P who required morphine (p < 0.001).
The total tramadol consumption did not differ between the groups during the first 7
Surgical outcomes
16/19 patients in group A and 9/19 in group P (p = 0.04) could walk with a frame at 6 hours
There was a difference between Group A and P in knee extension and knee flexion at 27 h
postoperatively 5(0-20) vs. 10(0-20) degrees (p=0.002) and 90(75-110) vs. 80(45-100)
degrees (p=0.001), respectively (Table 2). No statistically significant differences were found
between the groups at 3 days, 3 and 6 months postoperatively.
The median values of patient satisfaction scores varied between 3 and 4 and did not differ
between the groups at 24 hours and at 7 days. There was a statistically significant difference
in Oxford Knee Score at 3 months between the groups, with higher scores in group A than in
group P. No statistically significant difference in EQ-5D value was found postoperatively at 6
Adverse effects
There were no major surgical complications in any patient.
There was higher incidence of nausea (10 vs. 4), pruritus (4 vs. 0) and sedation (4 vs. 0) in
group P than in group A respectively (p<0.05).
There were 3 positive isolated cultures of the catheter tips, all with coagulase negative
staphylococcus. The patient in Group A with positive isolated culture had an increased CRP
of short duration without any increase of leucocytes. No antibiotic therapy was given and no
clinical signs of infection were found during the follow up period. The other 2 patients in
Group P had no increase in CRP or leucocytes. No patient was readmitted for any
complications to the hospital during the 6 months follow up.
Discussion
In one recent study on total knee arthroplasty, continuous femoral nerve block was compared
with the LIA-technique (Toftdahl et al. 2007). The authors found opioid consumption as well
as improved pain scores in the LIA group. When correctly performed by experienced
anesthesiologists, nerve blocks may be a good alternative to prolong postoperative pain relief.
However, the simplicity of LIA and its high success rate could be an advantage over
peripheral nerve blocks in this setting.
Unicompartmental arthroplasty with minimal invasive technique results in less operative
trauma in comparison with total knee arthroplasty. However, moderate-severe pain remains a
common problem. In an open pilot study (Beard et al. 2002) and a single blind study (Reilly et
al. 2005), a modified LIA-technique with only infiltration of ropivacaine, ketorolac and
adrenaline intraoperatively was tested during unicompartmental arthroplasty with promising
results. The infiltration technique in combination with oral NSAID´s and opioids resulted in
high patient satisfaction, good pain relief, and early discharge with no major complications. In
both studies, Redivac drain was used during the first 14-18 hours. In contrast to the above
studies, we have tested the LIA-technique in a double-blind study when a combination of
ropivacine, ketorolac and adrenaline were administered both intraoperatively and as well as
on day 1 postoperatively without postoperative Redivac drain. Both the intraoperative
infiltration and the postoperative intraarticular injection via the catheter of this combination of
analgesics resulted in good pain relief during the initial postoperative period and an increased
range of knee movement resulting in an early discharge. In addition to better pain relief, we
also found a lower consumption of rescue analgesics, which in turn resulted in a lower
incidence of opioid related side effects including sedation, pruritus and nausea when LIA was
One consequence of better pain relief is naturally improved mobilization. This can, however,
sometimes have detrimental effects as was seen in a study by Lombardi (Lombardi et al.
2004) on total knee arthroplasty who found a “rebound effect” on postoperative pain during
the first 2 postoperative days in the intervention group. Possible explanation for this finding
may include higher activity levels obtained by better pain control and less sedation, which in
turn could result in increased pain subsequently. Alternatively, patients may experience a
delay in the onset of pain levels postoperatively, which can be interpreted as greater pain
intensity. In our study we could not find such a rebound effect resulting in increased analgesic
Although good analgesia can be achieved using different techniques, it is important that
hospital stay is not prolonged. Thus, our aim was to achieve good pain relief and early
mobilization without prolonging recovery or hospital discharge. We used an objective method
to assess home-readiness since hospital discharge can be affected by several non-medical
factors and we informed the patients of the prospect of early discharge. These criteria have
been used by other authors as a way of objectively assessing recovery and discharge (Gupta et
al. 1999). Our findings show that there was a substantial reduction in hospital stay without
affecting patient satisfaction negatively. Others have reported similar results (Reilly et al.
Although pain relief was better in the LIA group, this did not translate into improved knee
function except at 27 h postoperatively. This could be explained in several ways. The scales
used for assessment of knee function may not be sensitive enough to detect differences after
knee surgery. Discharge time used in an appropriate way seemed to be a valuable tool.
Functional assessment by Oxford Knee Score should have been done earlier postoperatively
instead of after 2 weeks when pain intensity was low, even in the placebo group, which may
explain the absence of any differences between the groups.
We found no differences between the groups in the EuroQol preoperatively and after 6
months. Thus, data from both instruments measuring the functional assessment support the
findings of others that early discharge is safe and unicompartmental techniques (Beard et al.
2002, Reilly et al. 2005, Berend and Lombardi 2007).
We used a combination of ropivacaine, ketorolac and epinephrine for LIA. It is possible that a
combination of LA and ketorolac would have been adequate to provide similar pain relief.
However, we injected 200 mg ropivacaine locally and we were somewhat concerned about
LA toxicity due to the rapid absorption of ropivacaine from tissue planes. In addition,
adrenaline has been shown to have an alpha-2 agonistic effect similar to clonidine (Niemi and
Breivik 2002) and we thought that we might be able to further reduce pain by using this
Although the use of oral non-steroidal anti-inflammatory drugs (NSAID) in a multi-modal
analgesic regime may have further reduced pain intensity and rescue analgesic consumption,
we decided not to use these for several reasons. We used ketorolac as a part of the multimodal
analgesic technique with LIA which has previously been found to be efficacious (Beard et al.
2002, Reilly et al. 2005, Toftdahl et al. 2007). However, its combination with another oral
NSAID may result in systemic toxicity. Additionally, regional NSAID injections have been
shown to provide better analgesia in comparison to when they are administered systemically
We conclude that the LIA-technique could be recommended as a sufficient postoperative
analgesic technique after unicompartmental knee arthroplasties. More studies would be
valuable to investigate the best components in the mixture of drugs to be used in the LIA-
Contributions of authors
Designing the protocol and writing of document: PE, KA, AG. Enrolment of patients and
surgery: PE. Data collection: JK, ÖW. Data analysis: KA, AL, PE, AG. All authors
contributed towards the writing of the manuscript.
Acknowledgements
We thank Dr Kerr for his valuable information on the LIA- technique. The authors would also
like to thank the personnel in the operating theatres and postoperative and general orthopedic
wards for their constant enthusiasm during various phases of this study. We would also extend
our sincere appreciation to Anders Magnuson, Department of Epidemiology and Statistics for
References
Axelsson K, Johanzon E, Essving P, Weckstrom J, Ekback G. Postoperative extradural
analgesia with morphine and ropivacaine. A double-blind comparison between placebo and
ropivacaine 10 mg/h or 16 mg/h. Acta Anaesthesiol Scand 2005; 49: 1191-9.
Beard D J, Murray D W, Rees J L, Price A J, Dodd C A. Accelerated recovery for
unicompartmental knee replacement--a feasibility study. Knee 2002; 9: 221-4.
Berend K R, Lombardi A V, Jr. Liberal indications for minimally invasive oxford unicondylar
arthroplasty provide rapid functional recovery and pain relief. Surg Technol Int 2007;
Carlsson L V, Albrektsson B E, Regner L R. Minimally invasive surgery vs conventional
exposure using the Miller-Galante unicompartmental knee arthroplasty: a randomized
radiostereometric study. J Arthroplasty 2006; 21: 151-6.
Fransen M, Edmonds J. Gait variables: appropriate objective outcome measures in rheumatoid
arthritis. Rheumatology (Oxford) 1999; 38: 663-7.
Gupta A, Axelsson K, Allvin R, Liszka-Hackzell J, Rawal N, Althoff B, Augustini B G.
Postoperative pain following knee arthroscopy: the effects of intra-articular ketorolac
and/or morphine. Reg Anesth Pain Med 1999; 24: 225-30.
Jahromi I, Walton N P, Dobson P J, Lewis P L, Campbell D G. Patient-perceived outcome
measures following unicompartmental knee arthroplasty with mini-incision. Int
Kerr D R, Kohan L. Local infiltration analgesia: a technique for the control of acute
postoperative pain following knee and hip surgery: a case study of 325 patients. Acta
Lombardi A V, Jr., Berend K R, Mallory T H, Dodds K L, Adams J B. Soft tissue and intra-
articular injection of bupivacaine, epinephrine, and morphine has a beneficial effect
after total knee arthroplasty. Clin Orthop Relat Res 2004: 125-30.
McNamee D A, Parks L, Milligan K R. Post-operative analgesia following total knee
replacement: an evaluation of the addition of an obturator nerve block to combined
femoral and sciatic nerve block. Acta Anaesthesiol Scand 2002; 46: 95-9.
Niemi G, Breivik H. Epinephrine markedly improves thoracic epidural analgesia produced by
a small-dose infusion of ropivacaine, fentanyl, and epinephrine after major thoracic or
abdominal surgery: a randomized, double-blinded crossover study with and without
epinephrine. Anesth Analg 2002; 94: 1598-605, table of contents.
Reilly K A, Beard D J, Barker K L, Dodd C A, Price A J, Murray D W. Efficacy of an
accelerated recovery protocol for Oxford unicompartmental knee arthroplasty--a
randomised controlled trial. Knee 2005; 12: 351-7.
Reuben S S, Connelly N R. Postoperative analgesia for outpatient arthroscopic knee surgery
with intraarticular bupivacaine and ketorolac. Anesth Analg 1995; 80: 1154-7.
Rostlund T, Kehlet H. High-dose local infiltration analgesia after hip and knee replacement--
what is it, why does it work, and what are the future challenges? Acta Orthop 2007;
Toftdahl K, Nikolajsen L, Haraldsted V, Madsen F, Tonnesen E K, Soballe K. Comparison of
peri- and intraarticular analgesia with femoral nerve block after total knee
arthroplasty: a randomized clinical trial. Acta Orthop 2007; 78: 172-9.
Wang H, Boctor B, Verner J. The effect of single-injection femoral nerve block on
rehabilitation and length of hospital stay after total knee replacement. Reg Anesth Pain
Legends to figures
Day 1 represents the first postoperative day.
Group A (Active)= intraoperative, periarticular infiltration: 200 mg ropivacaine, 30mg
ketorolac and 0.5 mg epinephrine; postoperative, intraarticular injection: 150 mg ropivacaine,
Group P (Placebo)= no intraoperative infiltration and postoperative, intraarticular injection:
The median discharge times are shown: Group A = day 1 and in Group P = day 3 (p<0.001);
Number of patients discharged after 2 days: 17/19 in Group A vs. 6/19 in Group P (p<001).
Fig 3. Postoperative pain at rest. VAS-scores are presented as median and interquartile range
Fig 4. Postoperative pain on movement. VAS-scores are presented as median and interquartile
range (IQR). * p<0.001 (6 h); p<0.001 (12 h); p<0.001 (22 h); p=0.001 (27 h).
Assessed for eligibility Excluded (n = 17)
− Previous intubation difficulties (n = 1)
Randomized Group A (n = 20) Group P (n = 20) Excluded (n = 1) Intraoperatively Excluded (n = 1) 2 1 h postoperatively Figure 2
Number of patients discharged from hospital
Table 1
Demographic data and duration of surgery. Mean (SD)
Group A Group P Female/male (n) Weight (kg) Height (cm) ASA physical status I/II Operation time (min)
Group A (Active)= intraoperative, periarticular infiltration.
Group P (Placebo)= no intraoperative infiltration.
ASA physical status I= normal health; ASA physical status II= mild systemic disease.
Table 2 Mobilization and patient satisfaction
Knee extension (degrees) Preop
Knee flexion (degrees) Preop
Patient satisfaction 1 day postop
Oxford Knee Score Preop
EQ-5D Preop
n: number of patients who participated, varies due to patients´ ability to cooperate.
Knee extension and Knee flexion: Significant difference between the groups at 27 h.
Oxford Knee Score: 12 (the best possible) to 60 (the worst possible).
Preop score vs. 14 days postop scores: p= 0.05 (Group A); p < 0.001 (Group P).
Preop score vs. 3 months and 6 months postop. scores p=0.001 (Group A); p<0.001
EQ-5D Health outcome: 1=perfect health; 0= poor health and negative values= very poor
Preop values vs. 6 month values: p=0.001 (GroupA); p< 0.001( Group P).
http://www.state.il.us/court/Opinions/SupremeCourt/2002/June/Opinions/Html/88663.htmDocket No. 88663-Agenda 2-January 2002. THE PEOPLE OF THE STATE OF ILLINOIS, Appellee, v. DOROTHY WILLIAMS, Appellant. JUSTICE FREEMAN delivered the opinion of the court:In the circuit court of Cook County a jury convicted defendant, Dorothy Williams, of the robbery and murder of Mary Harris. Defendant waived a
Hugo Pena Brandão e Carla Patricia Bahry Gestão por competências: métodos e técnicas para mapeamento de competências Hugo Pena Brandão e Carla Patricia Bahry Introdução A gestão por competências tem sido apontada como modelo gerencialalternativo aos instrumentos tradicionalmente utilizados pelas organizações. Baseando-se no pressuposto de que o domínio de certos