Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Microsoft word - prostate enlargement.doc
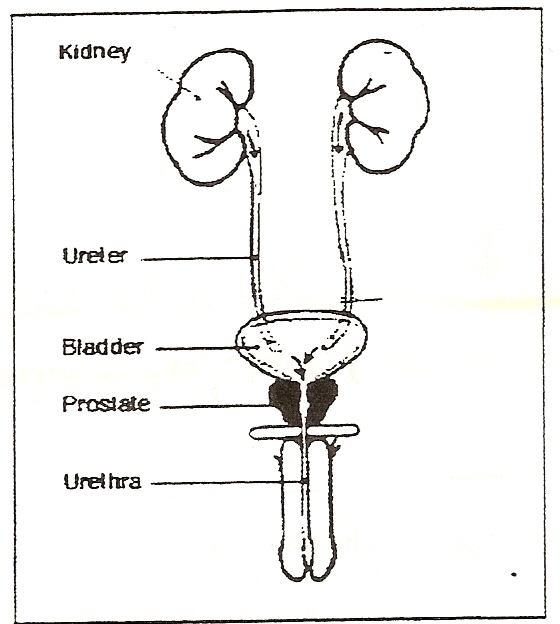
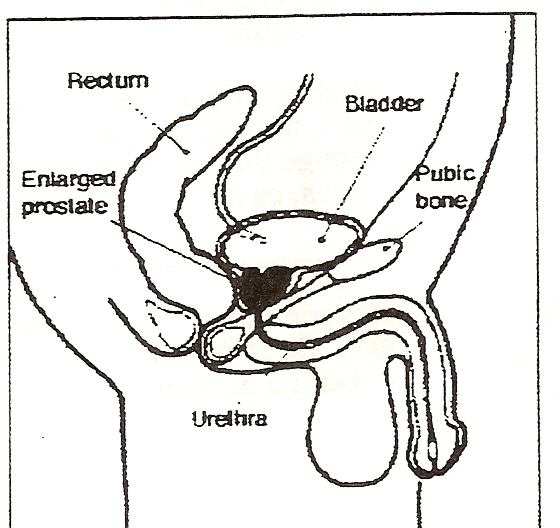
Prostate Enlargement BENIGN PROSTATIC HYPERPLASIA The Prostate Gland The prostate is a walnut-sized gland that forms part of the male productive system. The gland is made of two lobes, or regions, enclosed by an outer layer of tissue. As the diagrams show, the prostate is located in front of the rectum and just below the bladder, where urine is stored. The prostate also surrounds the urethra, the canal through which urine passes out of the body.
Scientists do not know all the prostate functions. One of its main roles, though, is to squeeze fluid into the urethra as sperm move through during sexual climax. This fluid, which helps make up semen, energizes the sperm and makes the vaginal canal less acidic. BPH: A Common Part of Aging It is common for the prostate gland to become enlarged as
ages. Doctors call the condition benign Prostatic hyperplasia (BPH) or benign prostatic hypertrophy.
Normal urine flow As a man matures, the prostate goes through two main periods of growth. The first occurs early in puberty, when the prostate doubles in size. At around age 25, the gland begins to grow again. This second growth phase often results, years later, in BPH. Though the prostate continues to grow during most of a man’s life, the enlargement doesn’t usually cause problems until late in life. BPH rarely causes symptoms before age 40, but more than half of men in their sixties and as many as 90 percent in their seventies and eighties have some symptoms of BPH. Urine flow with BPH
As the prostate enlarges the layer of tissue surrounding it stops it from expanding, causing the gland to press against the urethra like a clamp on the a garden hose. The bladder wall becomes thicker and irritable. The bladder begins to contract even when it contains small amount of urine, causing more frequent urination. Eventually, the bladder weakens and loses the ability to empty itself. Urine remains in the bladder. The narrowing of the urethra and partial emptying of the bladder cause many of the problems associated with BPH. Many people feel uncomfortable talking about the prostate, since the glands play a role in both sex and urination. Still, prostate enlargement is as common a part of aging as gray hair. As life expectancy rises, so does the occurrence of BPH. In the United States alone, 375,000 hospitals stays each year involve in a diagnosis of BPH. It is not clear whether certain groups face a greater risk of getting BPH. Studies done over the years suggest that BPH occurs more often among married men than single men and is more common in the United States and Europe than in other parts of the world. However, these findings have been debated, and no definite information on risk factors exists. In order to rule out cancer as a cause of urinary symptoms, your doctor may recommend a PSA blood test. PSA, a protein produced by prostate cells, is frequently present at elevated levels in the blood of men who have prostate cancer. The U.S. Food and Drug Administration has approved a PSA test for use in conjunction with a digital rectal exam to help detect prostate cancer in men age 50 or older and for monitoring prostate cancer patients after treatment. However, much remains unknown about the interpretation of PSA levels, the test’s ability to discriminate cancer from benign prostate conditions, and the best course of action following a finding of elevated PSA.
Because many unanswered questions surround the issue of PSA screening, the relative magnitude of its potential risks and benefits is unknown. Both PSA and ultra sound tests enhance detection when added to DRE screening. But they are known to have relatively high false-positive rates, and they may identify a greater number of medically insignificant tumors. Thus, PSA screening might lead to treatment of unproven benefit that could result in morbidity (including impotence and incontinence) and mortality. It cannot be determined from earlier studies whether PSA screening will reduce prostate cancer mortality. Ongoing studies are addressing this issue.
Rectal Ultrasound If there is a suspicion of prostate cancer, your doctor may recommend a test with rectal ultrasound. In this procedure, a probe inserted in the rectum directs sound waves at the prostate. The echo patterns of the sound waves form an image of the prostate gland on a display screen. Urine Flow Study Sometimes the doctor will ask a patient to urinate into a special device, which measures how quickly the urine is flowing. A reduced flow often suggests BPH. Intravenous Pyelogram (IVP) IVP is an x-ray of the urinary tract. In this test, a dye is injected into the vein, and the x-ray is taken. The dye makes the urine visible on the x-ray and shows any obstruction or blockage in the urinary tract. Cystoscopy In this exam, the doctor inserts a small tube through the opening of the urethra in the penis. This procedure is done after a solution numbs the inside of the penis so all sensation is lost. The tube, called a cystoscopy, contains a lens and a light system, which help the doctor see the inside of the urethra and the bladder. This test allows the doctor to determine the size of the gland and identify the location and the degree of the obstruction. Symptoms
Many symptoms of BPH stem from obstruction of the urethra and gradual loss of bladder function, which results in incomplete emptying of the bladder. The symptoms of BPH vary, but the most common ones involve changes or problems with urination, such as A hesitant, interrupted, weak stream. Urgency and leaking or dribbling. More frequent urination, especially at night. The size of the prostate does not always determine how the severe obstruction or the symptoms will be. Some men with greatly enlarged glands have little obstruction and few symptoms while others, whose glands are less enlarged, have more blockage and greater problems. Sometimes a man may not know he has any obstruction until he suddenly finds unable to urinate at all. This condition, called acute urinary retention, may be triggered by taking over- the-counter cold or allergy medicines. Such medicines contain a decongestant drug, known as a sympathomimetic. A potential side effect of this drug may be to prevent the bladder opening from relaxing and allowing urine to empty. When partial obstruction is present, urinary retention also can be brought on by alcohol, cold temperatures, or a long period of immobility. It is important to tell your doctor about urinary problems such as those described above. In 8 out of 10 cases, these symptoms suggest BPH, but they can also signal other, more serious conditions that require prompt treatment. These conditions, including prostate cancer, can be ruled out only by a doctor’s exam.
Severe BPH can cause serious problems over time. Urine retention and strain on the bladder can lead to urinary tract infections, bladder or kidney damage, bladder stones, and incontinence. If the bladder is permanently damage, treatment for BPH may be ineffective. When BPH is found in its earlier stages, there is a lower risk of developing such complications. Diagnosis
You may first notice symptoms of BPH yourself, or your doctor may find that your prostate is enlarged during a routine checkup. When BPH is suspected, you may be referred to a urologist, a doctor who specializes in problems of the urinary tract and the male reproductive system. Several tests help the doctor to identify the problem and decide whether surgery is needed. The tests vary from patient to patient, but the following are the most common. Digital Rectal Exam (DRE) This exam is usually the first test done. The doctor inserts a gloved finger into the rectum and feels the part of the prostate next to the rectum. This exam gives the doctor a general idea of the size and condition of the gland. Prostate Specific Antigen (PSA) Blood Test Drug Treatment Over the years, researchers have to find a way to shrink or at least stop the growth of the prostate without using surgery. Recently, several new medications have been tested in clinical trials, and the Food and Drug Administration (FDA) has approved four drugs to treat BPH. These drugs may relieve common symptoms associated with an enlarged prostate. Finasteride (marketed under the name Proscar), FDA-Approved in 1992, inhibits production of the hormone DHT, which is involved with prostate enlargement. Its use can actually shrink the prostate in some men. FDA also approved the drugs terazosin (marketed as Hytrin) in 1993, doxazosin (marketed as Cardura) in 1995, and Tamsulosin (marketed as Flomax) in 1997 for the treatment of BPH. All three drugs act by relaxing the smooth muscle of the prostate and bladder neck to improve urine flow and to reduce bladder outlet obstruction. Terazosin, doxazosin, and tamsulosin belong to the class of drugs known as alpha-blockers. Terazosin anddoxazosin were developed first to treat high blood pressure. Tamsulosin is the first alpha-blocker developed specifically to treat BPH. Surgical Treatment` Most doctors recommend removal of the enlarged part of the prostate as the best long-term solution for patients with BPH. With surgery for BPH, only the enlarged tissue that is pressing against the urethra is removed; the rest of the inside tissue and the outside capsule are left intact.
Surgery usually relieves the obstruction and incomplete emptying caused by BPH. The following section describes the types of surgery that are used. Transurethral Surgery. In this type of surgery, no external incision is needed. After giving anesthesia, the surgeon reaches the prostate by inserting an instrument through the urethra. A procedure called TURP (transurethral resection of the prostate) is used for 90 percent of all prostate surgeries done for BPH. With TURP, an instrument called a resectoscope is inserted through the penis. The resectoscope, which is about 12 inches long and ½ inch in diameter, contains a light, valves for controlling irrigating fluid, and an electrical loop that cuts tissue and seals blood vessels. During the 90- minute operation, the surgeon uses the resectoscope’s wire loop to remove the obstructing tissue one piece at a time. The pieces of tissue are carried by the fluid into the bladder and then flushed out at the end of the operation. Most doctors suggest using TURP whenever possible. Transurethral procedures are less traumatic than open forms of surgery and require a shorter recovery period. Your Recovery After Surgery
if you have surgery, you’ll probably stay in the hospital from 3 to 10 depending on the typ of surgery, you had and how quickly you recover.
Customer advice on sports injuries from Worcester Physiotherapy Clinic Cortisone is a type of steroid that is produced naturally by a gland in your body called the adrenal gland. Cortisone is released from the adrenal gland when your body is under stress. Natural cortisone is released into the blood stream and is relatively short-acting. Injectable cortisone is a synthetic (man made) drug a
502001 Rev E 04-29-13 Gold Standard Orthopaedics, LLC WARNINGS : The safety and effectiveness of pedicle screw spinal systems have been established only for spinal conditions with significant mechanical instability or deformity requiring fusion with instrumentation as described in the INDICATIONS Section. The safety and effectiveness of this device for any other conditions a
 Prostate Enlargement
Prostate Enlargement