Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Prostate gland enlargement
Prostate Gland Enlargement Benign Prostatic Hyperplasia
This leaflet only deals with benign (non-cancerous) enlargement of the prostate. Cancer of the prostate is a separate condition and is dealt with in another leaflet. What is the prostate gland?
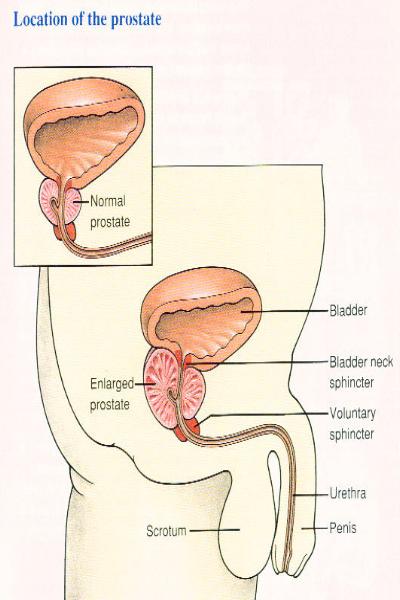
The prostate gland (just called 'prostate' from now on) is only found in men. It lies just beneath the bladder (see diagram). It is normally about the size of a chestnut. The urethra (the tube which passes urine from the bladder) runs through the middle of the prostate. The prostate helps to make semen, but most semen is made by the seminal vesicle (another gland nearby). The prostate gets bigger ('enlarges') gradually after the age of about 50. By the age of 70, about 8 in 10 men have an enlarged prostate. So, in later life it is as normal for your prostate to enlarge as it is to have grey hair. What are the symptoms of prostate enlargement?
About 1 in 3 men aged over 50 have some symptoms due to an enlarged prostate. As the prostate enlarges it may cause narrowing of the first part of the urethra. This may partially obstruct the flow of urine from the bladder. This can lead to 'obstructive' symptoms such as: Poor stream The flow of urine is weaker and it takes longer to empty your bladder. Hesitancy You may have to wait at the toilet for a while before urine starts to flow. Dribbling Some urine may trickle out and stain underpants soon after finishing at the toilet. Poor Emptying You may have a feeling of not quite emptying your bladder. The enlarged prostate may also 'irritate' the urethra and lower bladder which may cause: Frequency (passing urine more often than normal). This can be most irritating if it happens at night. Getting up several times a night is a common symptom and is called 'nocturia'. Urgency. This means you have to get to the toilet quickly when you 'need to go'. Usually the symptoms are mild to begin with. Perhaps a slight reduced urine flow or having to wait a few seconds to start passing urine. Over months or years the symptoms may become more troublesome and severe. Complications develop in some cases. Note 1: An enlarged prostate does not always cause symptoms. Also, the severity of the symptoms is not always related to the size of the prostate. It depends on how much the prostate presses on the urethra and lower bladder. Note 2: Not all urinary symptoms in men are due to an enlarged prostate. In particular, if you pass blood or have pain it may be due to bladder, kidney, or other prostate conditions. You should see a doctor if these symptoms occur, or if there is a change from your usual prostate symptoms. The prostate gland commonly becomes larger in older men. This is called Benign Prostatic Hyperplasia. It can cause problems with passing urine. Symptoms are often mild. Without treatment, symptoms do not always get worse, and may even improve over time. If symptoms become troublesome or distressing they can often be improved by medicines or surgery. What are the possible complications?
Complications are not common, but include the following: In some cases a sudden total blockage of urine occurs. This is called 'acute urinary
retention'. It is very distressing and you need emergency treatment to drain the bladder. It occurs in less than 1 in 100 men with an enlarged prostate each year. It is more common if you have fairly troublesome symptoms already. However, in some cases, it can develop 'out of the blue' in a man who has not previously had any prostate-related symptoms
In some cases, only some of the urine in the bladder is emptied when you pass urine. Some
urine remains in the bladder at all times. This is called 'chronic (ongoing) retention'. This may cause recurring urine infections, or incontinence (as urine dribbles around the blockage rather than large amounts being passed each time you go to the toilet)
There is a small increased risk of developing sexual problems. For example, difficulty with
getting an erection, pain on ejaculation, and reduced amount of semen when you ejaculate. It is not clear how an enlarged prostate may cause these problems in some cases
Note: the risk of prostate cancer is not increased. Men with a benign prostate enlargement are no more or less likely to develop prostate cancer than those without benign prostate enlargement. Do I need any tests? A doctor may examine your prostate to see how big it is. This is done by a doctor placing a
gloved finger inside your anus to feel the prostate from behind
A urine and blood test may be done to check the function of your kidneys, and to rule out
other causes of passing urine frequently (such as diabetes or a urine infection)
A referral to a bladder specialist (urologist) may be advised if symptoms are severe, or if
complications develop. Tests may be done in these more severe cases, particularly if surgery is being considered as a treatment. For example; cystoscopy (a look inside the bladder with a special telescope); a urine flow test to assess how bad the obstruction has become; a scan to see whether much urine remains in the bladder after you pass urine
A PSA (Prostate Specific Antigen) blood test may be offered. This can be used as a 'marker'
for the size of the prostate. Larger prostates make more PSA.
(Note: a high PSA level is found in people with prostate cancer. It has to be stressed that most men with prostate symptoms do not have prostate cancer. The result of the PSA test needs to be interpreted by a doctor who takes into account various factors such as your age, size of prostate, etc.) Is treatment always necessary?
No. In most cases, an enlarged prostate does not do any 'damage' or cause complications. Whether treatment is needed usually depends on how much bother the symptoms cause. For example, you may be glad for some treatment if you are woken six times a night, every night, with an urgent need to go to the toilet. On the other hand, slight hesitancy when you go to the toilet and getting up once a night to pass urine may cause little problem and not need treatment. What are the treatment options for prostate enlargement? Not treating may be an option (often called 'watchful waiting')
If symptoms are mild then this may be the best option. You may be happy to just 'see how things go' if the symptoms are not too bothersome and are not affecting your life very much. The situation can be reviewed every year or so, or sooner if there is change in symptoms. Symptoms do not always become worse. They may even improve. One study of men with moderate symptoms who had no treatment, but were followed up for five years found: in 9 out of 20 cases, the symptoms remained about the same in 8 out of 20 cases, the symptoms improved (without treatment) in 3 out of 20 cases, the symptoms became worse
Medicines
The decision to treat with medicines usually depends on how much bother the symptoms are causing you. There are two types of medicines that may help - alpha-blockers and 5-alpha reductase inhibitors. Medicines do not cure the problem, nor do they usually make symptoms go completely. However, symptoms often ease if you take a medicine. Alpha-blocker medicines
There are several different types and brands of alpha-blockers which include: prazosin, indoramin, tamsulosin, alfuzosin, doxazosin and terazosin. These medicines work by relaxing the muscle tissue of the prostate and at the outlet of the bladder. In most cases, symptoms improve with taking an alpha-blocker. However, the amount of improvement varies from person to person. Some improvement usually occurs within a few days, but the full effect may take 4-6 weeks. Most men can take an alpha-blocker without any problems, but side-effects occur in some cases. These include: slight drowsiness, headaches, and dizziness. (Read the leaflet in the medicine packet for a full list of possible side-effects.) 5-alpha reductase inhibitor medicines
These are alternatives to alpha-blockers. There are two types - finasteride and dutasteride. These medicines work by blocking the conversion of the hormone testosterone to dihydrotestosterone in the prostate. They do this by blocking an enzyme (chemical) called 5- alpha-reductase. Dihydrotestosterone is partly responsible for making the prostate enlarge. Therefore, a reduced amount of dihydrotestosterone in the prostate tends to cause it to shrink. On average, finasteride or dutasteride can cause the prostate to shrink by about 30%. Symptoms may improve as the prostate becomes smaller. The full effect can take up to six months as the prostate gradually shrinks. As with alpha-blockers, the amount of improvement with finasteride or dutasteride varies from person to person, and no improvement occurs in some cases. Side-effects sometimes occur with these medicines. Two examples are impotence and reduced sex drive. These occur in up to 1 in 20 men who take finasteride or dutasteride, but are reversible if the medication is stopped. (Read the leaflet in the medicine packet for a full list of possible side effects.) Which medicine is chosen?
The severity of symptoms is not always related to the size of the prostate. A small or large enlargement may cause mild or severe symptoms. An alpha-blocker may help whatever the
size of the prostate, as it works by relaxing muscle fibres. Finasteride or dutasteride tend to work best if you have a particularly large prostate which has more tissue to shrink. Your doctor will advise which medicine may be best in your circumstances. Also, if you develop a problem or side-effect with one type of medicine, then another type may be an option. Combinations of medicines
In some cases, a combination of an alpha blocker plus a 5-alpha reductase inhibitor is used. This may give quicker and better relief of symptoms than either alone. Some studies suggest that in men who take a combination of two medicines, about 4 in 5 can stop the alpha-blocker after 6-12 months without their symptoms getting any worse. This is likely to be because the prostate will have shrunk with the 5-alpha reductase inhibitor after this time, and the alpha-blocker is no longer then needed. Herbal remedies
Herbal remedies that you can buy for an enlarged prostate include: Saw Palmetto, Beta Sitosterol Plant Extracts, Rye Grass, and Pygeum Africanum Bark Extract. These are sometimes heavily advertised, but there is little scientific evidence that they work well. Saw Palmetto has some evidence that it helps, but it is not conclusive. It may be worth a try if symptoms are mild. Surgery
Removal of all, or part, of the prostate is an option if symptoms are very bothersome, or if medicines do not help. The common operation is called 'Trans Urethral Resection of Prostate' (TURP). In this operation the prostate is chipped away by an instrument that is passed up the urethra of the penis. This operation gives good improvement in symptoms in most cases. However, in a small number of cases, surgery does not improve the symptoms. In particular, in people with irritative symptoms (frequency and urgency - see above), approximately a third of them will continue to have some degree of symptoms after the operation. Also, complications occur in some cases. For example, after this operation about 1 in 10 men become impotent, and about 1 in 100 men become incontinent of urine. Also, more than half of men develop 'retrograde ejaculation'. This means that during sex, the semen ejaculates ('comes') into the bladder, and is passed out later with urine. As in all operations, there is a small risk of death. Other surgical techniques are being developed such as microwave shrinkage and laser treatment of the prostate. They are available at some centres. The role of these techniques is not yet fully established, but they may become more popular in the future.
Coping with symptoms of prostate enlargement
Treatment may not totally clear all symptoms, although they can usually be greatly improved. The following tips may help if you opt not to have treatment (for example if symptoms are mild) or if treatment does not fully work. Try to anticipate times when urinary frequency and urgency are likely to be most
inconvenient, and reduce the amount that you drink beforehand. For example, when you go out, don't drink much for 2-3 hours before you go out. However, do not reduce the total amount of fluid that you would normally drink each day
After you have finished passing urine, go back to the toilet again after a few minutes to try
and pass some more. (This is called double micturition.) This aims to make sure the bladder is emptied completely
Consider reducing or stopping caffeine (in tea, coffee, cola, etc) and alcohol. These can
make the symptoms of frequency, urgency, and nocturia worse
If hesitancy is a problem - try to positively relax when starting to pass urine. For example, try
If urgency is a problem - try some distraction techniques such as breathing exercises and
mental tricks (for example, counting) to take your mind off the bladder
If frequency is a problem - try retraining the bladder by 'holding on' for as long as you can
each time before passing urine. The bladder muscle can be trained to expand more in this way. Eventually, the bladder may be trained to hold on for longer each time before you need to go to the toilet
Further help and information Prostate Research Campaign UK 10 Northfields Prospect Putney Bridge Road London, SW18 1PE Tel: 020 8877 5840 Web: www.prostate-research.org.uk Prostate Help Association Langworth Lincoln LN3 5DF Web: www.pha.u-net.com Email or postal contact only. Please send two 1st class stamps for initial information.
HDW-650P HDCAM has become the format of choice around Features the world for high quality HD programming acrossa wide range of production genres. Since launchover 43,000 HDCAM camcorders and VTRs have Choice of HD Recording Formats, includ- been purchased, and year-by-year Sony has con- ing both interlaced and progressive tinued to strengthen the line-up to offer new cre-The HDW-650
 Note 2: Not all urinary symptoms in men are due to an enlarged prostate. In particular, if you
Note 2: Not all urinary symptoms in men are due to an enlarged prostate. In particular, if you