Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Pii: s0895-7061(00)01235-8
Device-Guided Breathing Exercises Reduce Blood Pressure: Ambulatory and Home Measurements
Talma Rosenthal, Ariela Alter, Edna Peleg, and Benjamin Gavish
Slow breathing practiced routinely using an interactive
older patients and higher baseline BP. The results provide
device has demonstrated a sustained reduction in high
additional support for the efficacy of the device as an
blood pressure (BP). We reevaluated the BP response of
adjunctive lifestyle modification for treating hypertension.
hypertensives (n ϭ 13) to this daily treatment for 8 weeks
Am J Hypertens 2001;14:74 –76 2001 American Journal
using 24-h ambulatory, home, and office BP measure-
ments. A clinically significant BP reduction of similarmagnitude was observed in all BP monitoring modalities
Key Words: Lifestyle modification, therapeutic, ambu-
during the daytime. Greater BP reductions were found for
latory blood pressure, hypertension. Thesideeffectsandcostofantihypertensivedrugs anddigitalBPmonitoring(BPM)performedathomein
have led to the search for effective nonpharmaco-
addition to standard office measurements.
logic treatment alone or as an adjunct to drug
therapy.1 Recently, a randomized controlled study re-
ported that device-guided slow breathing with prolonged
Subjects
expiration performed daily for 2 months resulted in a
The study population included 13 hypertensives, 7 men
sustained office blood pressure (BP) reduction of 16.2/
and 6 women, 6 medicated with antihypertensive drugs
10.6 mm Hg from a baseline BP of 158/97 mm Hg (n ϭ
with no dose change for 3 weeks before the study, and 7
65).2 A similar study with this device involved home BP
unmedicated, aged 25–75 years, excluding patients with
BP classified as stage III (systolic BP Ն180 mm Hg or
Breathing exercises play a prominent role in behavioral
diastolic BP Ն110 mm Hg) and unmedicated patients with
methods such as yoga, meditation, and biofeedback, which
have had some success in treating high BP.4–6 There may
Study Design
be some rationale for the therapeutic effect of the breathingexercises, as the acute response to slow and stable breath-
The study included only one treatment group. During the
ing includes a number of beneficial effects on the cardio-
study a patient visited the clinic five times. Visits 1 and 2,
vascular system, both at the systemic and the microvascu-
1 day apart, were used for eligibility and baseline office
lar level. These include increasing baroreflex sensitivity,
and 24-h ambulatory BP measurements. Treatment and
heart rate variability, microvascular flow and venous re-
home BP measurement took place during the next 8
turn, and reducing BP and peripheral resistance.7–11 How-
weeks. One follow-up visit (No. 3) was scheduled at the
ever, some of the observed antihypertensive effect elicited
end of 4 treatment weeks. Office and 24-h ambulatory BP
by the breathing exercises may be attributed to placebo
measurements were done at the end of treatment (visits 4
response, to which office BP measurements are sensitive,
and 5, 1 day apart). An assistant trained the patient in
but ambulatory and home BP monitor are relatively insen-
using the device and the home BP monitor during visit 2
It is the purpose of the present study to reevaluate the
Treatment
efficacy of the breathing-guiding device in reducing theBP of hypertensives using 24-h ambulatory BP monitoring
Treatment consisted of 15 min daily, breathing exercisesperformed for 8 weeks, musically guided by a device
Received May 25, 2000. Accepted June 6, 2000.
Address correspondence and reprint requests to Talma Rosenthal,
From the Chorley Hypertension Unit, Chaim Sheba Medical Center
MD, Chorley Hypertension Unit, Chaim Sheba Medical Center, Tel
(TR, EP), Tel Hashomer and InterCure Ltd. (AA, BG), Neve-Ilan, Israel.
Hashomer, Israel; e-mail: talros_il@yahoo.com
2001 by the American Journal of Hypertension, Ltd.Published by Elsevier Science Inc.AJH–January 2001–VOL. 14, NO. 1 DEVICE-GUIDED BREATHING REDUCES BLOOD PRESSURE
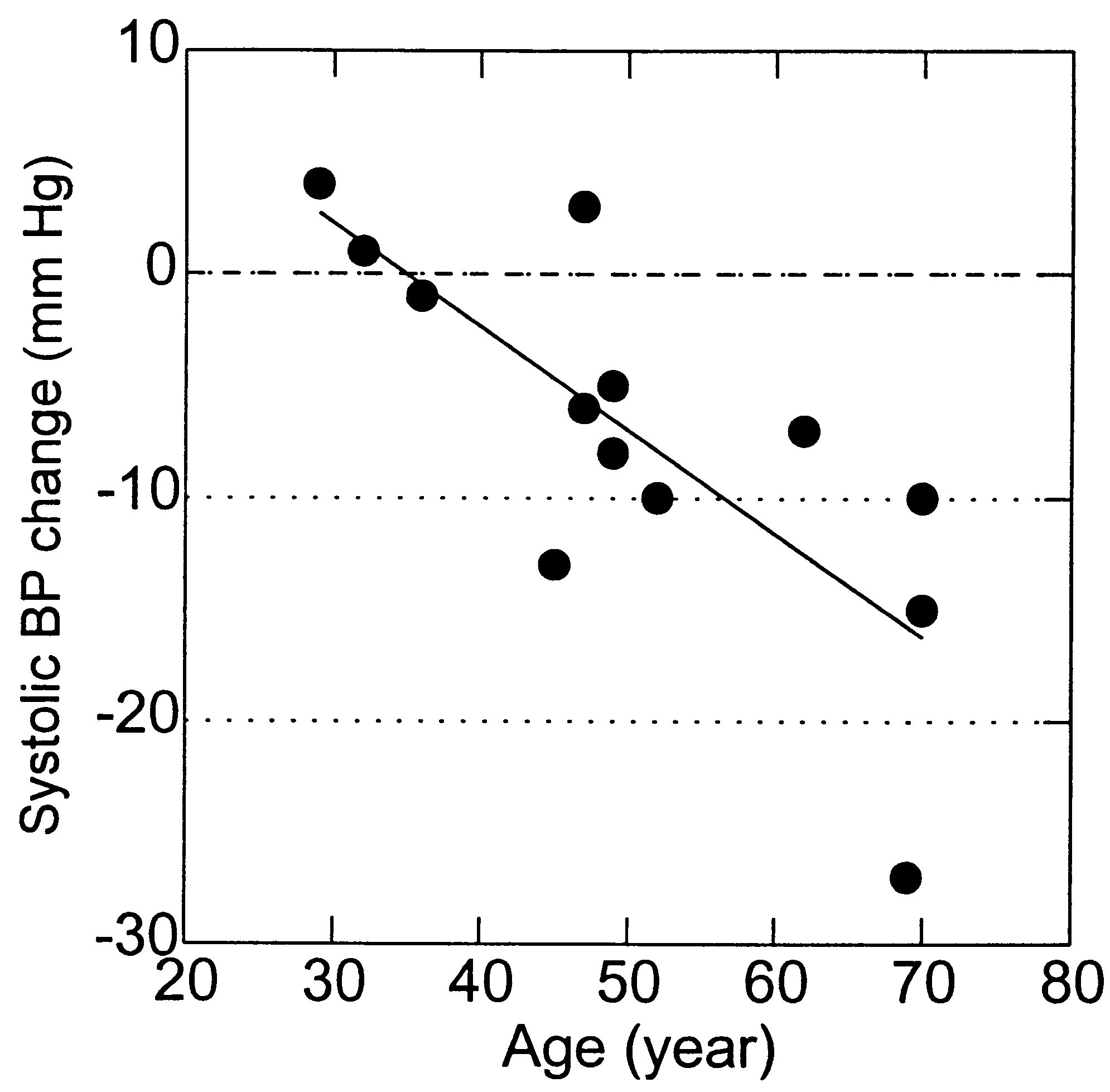
called Respi-Low (InterCure Ltd., Neve Ilan, Israel). Thedevice consists of a belt-type respiration-movement sensormounted on the upper abdomen or chest, attached to acomputerized control unit and headphones. On the basis ofan analyzed monitored breathing pattern, the device com-poses, in real-time, music-like sound patterns with a tem-poral structure similar to the actual breathing pattern butwith prolonged “expiration” (in the sound pattern). Thebreathing pattern modification occurs as the user volun-tarily follows the sound pattern with his or her breathingmovements. This process continues until a steady state isreached at the lowest breathing rate comfortable for theuser. The device also has a data logger that stores anddisplays data including date, time, and duration of use, andperformance parameters for the purpose of technical helpby telephone. The treatment took place at home, during theafternoon or evening. No change was made in the antihy-pertensive medication throughout the study period. Treat-ment started after visit 2 and stopped before visit 4. De-vices were then collected and downloaded. FIG. 1. Age dependence of change in 24-h ambulatory systolic BP Measurements
blood pressure (BP) (awake) in response to treatment. Each pointcorresponds to an individual patient. The regression line is marked.
Office BP was measured in a sitting position, after the
The correlation coefficient is r ϭ 0.76 and the slope is Ϫ0.46 mm
patient had rested for 5 min, using a standard procedure.
The BP level for each device was taken as the average ofthe last two readings after three consecutive readings. Twenty-four-hour ambulatory BP was determined at fre-
changes were tested for being different from zero by
quency of four per hour using Suntech Accutracker (Sun-
one-sample t test. Dependence of BP changes on age and
tech Medical Instruments, Raleigh, NC). The attached
baseline values were determined using linear regression
software provided the average BP in the awake and asleep
models, where the P values correspond to the regression
phases. Home BP was measured with Omron IC, a digital
coefficients (eg, the significance of a non-zero slope as
BPM that stores all data including BP, heart rate, date, and
illustrated in Fig. 1). All P values were two-tailed. Statis-
hour up to 350 measurements without a possibility to erase
tical significance was associated with P Ͻ .05.
or replace data by the user. Patients were instructed tomeasure BP in the morning three times consecutively in acomfortable sitting position after at least 5 min of rest, and
to refrain from smoking, physical exercise, or caffeine
Baseline characteristics (mean Ϯ SD) were age 50.5 Ϯ
during the 30 min preceding the measurement.
13.9 years and body mass index 25.0 Ϯ 5.2. Systolic/
Subject’s compliance with treatment was checked using
diastolic BP were the following: for 24-h ambulatory,
data stored in the data logger of the Respi-Low during the
137.1 Ϯ 6.9/82.5 Ϯ 8.4 mm Hg for awake (n ϭ 13) and
study (by telephone) and after the study, when the data
117.8 Ϯ 10.3/69.4 Ϯ 10.5 mm Hg for asleep (n ϭ 12).
files were downloaded. Compliance with home BP mea-
Office BP was 140.7 Ϯ 13.9/86.1 Ϯ 8.9 mm Hg and home
surements was checked by the dates and times of the
BP was 146.4 Ϯ 15.4/84.8 Ϯ 8.3 mm Hg. Heart rate was
measurements stored in the BPM and downloaded at visits
75.2 Ϯ 6.7 beats/min. The number of patients at each BP
classification was 1, 3, 7, and 2 for normal, high normal,
Data Analyses and Statistics
stage I, and stage II, respectively.
The response to treatment is summarized in Table 1. In
The study outcomes were the average systolic and dia-
general, BP changes were similar in all monitoring meth-
stolic BP changes from baseline level (visits 1 and 2 for
ods. Significant systolic BP reduction was observed in the
the office and 24-h ambulatory) to end level (visits 4 and
24-h ambulatory (awake) and the office BP. There was a
5). For the home measurements study outcomes were the
73% correlation between the 24-h ambulatory home mean
average daily BP in the first and last 2 weeks. Heart rate
arterial pressure (MAP) change (defined as: diastolic ϩ
changes were defined accordingly. The primary study out-
(systolic Ϫ diastolic)/3). No correlation was found be-
come was the 24-h ambulatory BP changes in the awake
tween office BP changes and baseline values of either
phase, as outcomes of previous studies (office BP changes)
ambulatory or home BP or the difference between office
were defined at this time phase. The BP and heart rate
and home BP, which discloses white coat effect. There was
DEVICE-GUIDED BREATHING REDUCES BLOOD PRESSURE AJH–January 2001–VOL. 14, NO. 1
office systolic BP change between the present and the
previous study can be explained quantitatively by its de-
BP Change (mm Hg)
pendence on the baseline BP, which was higher in the
BP Monitoring Modality (n Systolic Diastolic
In conclusion, the present study provides additional evi-
dence of the benefit of routine breathing exercises guided by
the tested device as a safe and efficacious adjunctive lifestyle
modification for treating hypertension. References
* P Ͻ .05. † P Ͻ .01.
The Joint National Committee on Prevention, Detection, Evaluation,
and Treatment of High Blood Pressure: The Sixth Report of theJoint National Committee on Prevention, Detection, Evaluation, andTreatment of High Blood Pressure. Arch Intern Med 1997;157:
no significant change in heart rate (Ϫ1.0 Ϯ 5.2 beats/min)
Schein M, Gavish B, Herz M, Rosner-Kahana D, Naveh P, Knish-kowy B, Zlotnikov E, Ben-Zvi N, Melmed RN: Self-treatment of
The BP reduction effect of the treatment was found to
hypertension with device-guided breathing exercises: a double-blind
increase with age in the ambulatory systolic BP (awake),
randomized study. J Human Hypertens 2000 (In press).
as shown in Fig. 1 and the corresponding MAP reduction
Grossman E, Grossman A, Schein MH, Zimlichman R, Gavish B:
(P ϭ .02). Using a similar analysis, MAP reduction at
Breathing-control lowers blood pressure (BP). J Human Hypertens
home was found to increase with age (P ϭ .05) and
Patel C, North WRS: Randomised controlled trial of yoga and
baseline home MAP (P ϭ .01), whereas office systolic
biofeedback in management of hypertension. Lancet 1975;ii;93–95.
BP reduction appears to increase for greater baseline sys-
Patel C, Margot MG, Terry DJ, Carruthers M, Hunt B: Trail of
relaxation in reducing coronary risk: four-year follow up. BMJ
The contribution of age and baseline BP level can be
demonstrated by calculating the MAP change for three
Irvine J, Johnson DW, Jenner D, Marie GV: Relaxation and stressmanagement in the treatment of essential hypertension. J Psycho-
groups: group I, all patients (n ϭ 13), group II, patients
aged Ն40 years old (n ϭ 9), and group III, patients with
de Daly MB: Interaction between respiration and circulation, in
baseline home MAP Ն 100 mm Hg (n ϭ 7). The MAP
Cherniak NS, Widdicombe JG (eds): Handbook of Physiology,
changes obtained with ambulatory (awake), home BP and
Section III, Volume 2, Part II. Bethesda, Am Physiol Soc, 1986, pp
office BP were, respectively, Ϫ3.9, Ϫ3.9, and Ϫ4.7 mm
de Daly MB: Aspects of the integration of the respiratory and
Hg (P Ͻ .05) for group I; Ϫ5.7, Ϫ5.8, and Ϫ4.8 mm Hg
cardiovascular system, in Jordan D, and Marshall J (eds): Cardio-
for group II (P Ͻ .05); and Ϫ5.1, Ϫ7.2, Ϫ6.4 (P Ͻ .01)
vascular Regulation. London, Portland, 1995, 15–35.
Pitzalis MV, Mastropasqua F, Massari F, Passantino A, Colombo R,Mannarini A, Forleo C, Rizzon P: Effect of respiratory rate on therelationship between RR interval and systolic blood pressure fluc-
Discussion
tuations: a frequency-dependent phenomenon. Cardiovasc Res1998;38:332–339.
In terms of the magnitude of BP reduction by accepted
10. Novak V, Novak P, de Champlain J, Nadeau R: Altered cardiore-
lifestyle modifications,14,15 the BP reduction achieved by
spiratory transfer in hypertension. Hypertension 1994;23:104 –113.
the treatment device is clinically significant. The similarity
11. Cooke WH, Cox JF, Diedrich AM, Tatlor A, Beighol LA, Ames IV
in BP response to treatment obtained with 24-h ambula-
JE, Hoag JB, Seidel H, Eckberg DL: Controlled breathing protocolsprobe human autonomic cardiovascular rhythms. Am J Physiol
tory, home, and office measurements suggests that the BP
reduction is not likely due to the placebo effect.12,13 The
12. Mutti E, Trazzi S, Omboni S, Parati G, Mancia G: Effect of placebo
increased BP reduction for greater age or greater baseline
on 24-h non-invasive ambulatory blood pressure. J Hypertens 1991;
BP, and the absence of any significant change in the heart
rate, are of considerable interest for two reasons. First, the
13. Vaur L, Dubroca I, Dutrey-Dupagne C, Genes N, Chatellier G,
Bouvier-d’Yvoire M, Elkik F, Menard J: Superiority of home blood
benefits of the treatment are greater for patients found at
pressure measurements over office measurements for testing. Blood
higher risk for cardiovascular disease, older or with a
higher BP. Second, these correlations may reflect a vas-
14. Dengel DR, Galecki AT, Hagberg JM, Pratley RE: The independent
cular property, that is, beneficially modified by the treat-
and combined effects of weight loss and aerobic exercises on blood
ment, such as arterial compliance, which is reduced in
pressure and oral glucose tolerance in older men. Am J Hypertens1998;11:1405–1412.
older age and higher BP. However, larger sample size and
15. Midgley JP, Matthew AG, Greenwood CMT: Effect of reduced
other vascular probes are needed before such speculation
dietary sodium on blood pressure: a meta-analysis of randomized
can be applied. It is noteworthy that the difference in the
controlled trials. JAMA 1996;275:1590 –1597.
VIRACEPT® (nelfinavir mesylate) TABLETS and ORAL POWDER ALERT: Find out about medicines that should NOT be taken with VIRACEPT . Please also read the section “MEDICINES YOU SHOULD NOT TAKE WITH VIRACEPT”. Patient Information VIRACEPT® (VI-ra-cept) Generic Name: nelfinavir (nel-FIN-na-veer) mesylate Please read this information carefully before taking VIRACEPT. Also, please read
CURRICULUM VITAE Dr. LUCA MERTEL Medico Veterinario, Dottore di Ricerca. DATI PERSONALI - Nato a Milano il 14 Novembre 1963. Si é laureato il 9 Novembre 1989 discutendo la tesi intitolata "La cheratocongiuntivite secca (KCS) nel cane" con la votazione di 110/110 e lode. Iscritto all’Ordine Provinciale dei Medici Veterinari di Milano dal 23 Gennaio 1990. Indirizzo e-mail: lucame
 AJH–January 2001–VOL. 14, NO. 1 DEVICE-GUIDED BREATHING REDUCES BLOOD PRESSURE
AJH–January 2001–VOL. 14, NO. 1 DEVICE-GUIDED BREATHING REDUCES BLOOD PRESSURE