11 Jul 2012
Peripheral arterial disease (PAD), also called peripheral vascular disease (PVD), is a narrowing of the arteries. It
mainly occurs in arteries that supply blood to the legs. The main symptom is pain in one or both legs when you
walk. Treatment usually includes: stopping smoking (if you smoke), regular exercise, medication to lower your
cholesterol level, a daily aspirin and lowering your blood pressure if it is high. Medicines to open up the arteries
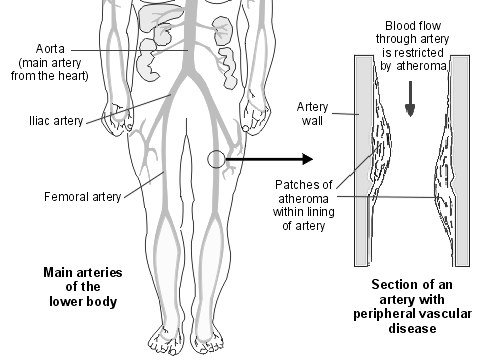
may help. Surgery may be needed in severe cases. What is peripheral arterial disease? Peripheral arterial disease (PAD) is narrowing of one or more arteries (blood vessels). It mainly affects arteries that take blood to your legs. (Arteries to the arms are rarely affected and are not dealt with further in this leaflet.) The condition is also known as peripheral vascular disease (PVD). It is also sometimes called hardening of the arteries of the legs.
In the UK, around 1 in 5 men and 1 in 8 women aged 50-75 years have PAD. It becomes more common with increasing age. What causes peripheral arterial disease? The narrowing of the arteries is caused by atheroma. Atheroma is like fatty patches (plaques) that develop within the inside lining of arteries. A patch of atheroma starts quite small, and causes no problems at first. Over the years, a patch of atheroma can become thicker. (It is a bit like scale that forms on the inside of water pipes.)
A thick patch of atheroma makes the artery narrower. This reduces the flow of blood through the affected section of artery. Tissues downstreamhave a reduced blood supply, which can lead to symptoms and problems. Atheroma can develop in any artery, but the common arteries affectedare:
Arteries taking blood to the heart - this is called ischaemic heart disease and may lead to problems such as angina and heart attacks.
Arteries taking blood to the brain - which may eventually lead to a stroke.
Arteries taking blood to the legs - which may lead to PAD. What causes atheroma? Everybody has some risk of developing atheroma. However, certain risk factors increase the risk. Risk factors include:
Lifestyle risk factors that can be prevented or changed:o
Lack of physical activity (a sedentary lifestyle).
Treatable or partly treatable risk factors:o
High triglyceride (fat) blood level.
Kidney diseases causing diminished kidney function.
Fixed risk factors - ones that you cannot alter:o
A strong family history. This means if you have a father or brother who developed heart disease or a stroke before they were aged55 years, or in a mother or sister before they were aged 65 years.
Age. The older you become, the more likely you are to develop atheroma.
Ethnic group. For example, people who live in the UK, with ancestry from India, Pakistan, Bangladesh or Sri Lanka, have anincreased risk.
However, if you have a fixed risk factor, you may want to make extra effort to tackle any lifestyle risk factors that can be changed. Note: some risk factors are more risky than others. For example, smoking causes a greater risk to health than obesity. Also, risk factors interact. So, having two or more risk factors has a much more increased risk compared with a person who only has one risk factor. For example, a middle-aged male smoker who does little physical activity and has a strong family history of heart disease has quite a high risk of developing a cardiovascular disease such as a heart attack, stroke, or PAD before the age of 60 years.
Research is looking at some other factors that may be risk factors. For example, high blood levels of apolipoprotein B or homocysteine arebeing investigated as possible risk factors. What are the symptoms of peripheral arterial disease? The typical symptom is pain which develops in one or both calves when you walk or exercise and is relieved when you rest for a few minutes. This pain varies between cases and you may feel aching, cramping or tiredness in your legs. This is called intermittent claudication. It is due to narrowing of one (or more) of the arteries in your leg. The most common artery affected is the femoral artery.
When you walk, your calf muscles need an extra blood and oxygen supply. The narrowed artery cannot deliver the extra blood and so pain occursfrom the oxygen-starved muscles. The pain comes on more rapidly when you walk up a hill or stairs than when on the flat.
If an artery higher upstream is narrowed, such as the iliac artery or aorta, then you may develop pain in your thighs or buttocks when you walk.
If the blood supply to the legs becomes worse, the following may be found by a doctor who examines you:
Poor hair growth below your knee and poor toenail growth.
Weak or no pulses in the arteries of your feet. Severe cases If the blood supply is very much reduced, then you may develop pain even at rest, particularly at night when the legs are raised in bed. Typically, rest pain first develops in the toes and feet rather than in the calves. Ulcers (sores) may develop on the skin of your feet or lower leg if the blood supply to the skin is poor. In a small number of cases, gangrene (death of tissue) of a foot may result. However, this is usually preventable (see below). How is peripheral arterial disease diagnosed? The diagnosis is usually made by the typical symptoms. A simple test that your doctor or nurse may do is to check the blood pressure in your ankle and compare this to the blood pressure in your arm. This is called the ankle brachial pressure index (ABPI). If the blood pressure in your ankle is much different to that in your arm then this usually means that one or more arteries going to your leg, or in your leg, are narrowed. However, the ABPI can be normal in some cases. Although this test can help your doctor find out if PAD is affecting your legs, it will not identify which blood vessels are blocked.
More sophisticated tests are not needed in most cases. They may be done if the diagnosis is in doubt, or if surgery is being considered (whichis only in the minority of cases). For example, a CT scan, an MRI scan or an ultrasound scan of the arteries can build up a map of your arteriesand show where they are narrowed. What is the outlook (prognosis) for peripheral arterial disease? Studies that have followed up people with PAD have shown that:
Symptoms remain stable or improve in about 15 out of 20 cases.
Symptoms gradually become worse in about 4 out of 20 cases.
Symptoms become severe in about 1 out of 20 cases.
So, in most cases, the outlook for the legs is quite good.
However, if you have PAD, it means that you have an increased risk of developing atheroma in other arteries. You have around a 6-7higher-than-average risk of developing heart disease (such as angina or a heart attack) or of having a stroke. The main concern for most peoplewith PAD is this increased risk of having a heart attack or stroke. Note: your chance of developing severe PAD (and heart disease or a stroke) is much reduced by the self-help measures and treatments described below. What self-help measures can I do? Stop smoking If you smoke, stopping smoking is the single most effective treatment. Stopping smoking increases walking distance by two or threefold in over 8 out of 10 people with PAD. (Stopping smoking also greatly reduces your risk of having a heart attack or stroke.)
You should see your practice nurse for help if you find it difficult to stop smoking. Nicotine gum or patches to help you stop may be an option. There are also other medicines that are sometimes prescribed to help people stop smoking. Exercise regularly Regular exercise encourages other smaller arteries in the legs to enlarge and improve the blood supply. If you exercise regularly, there is a good chance that symptoms will improve, and the distance that you can walk before pain develops will increase.
Walking is the best exercise if you have PAD. Regular exercise means a walk every day, or on most days. Walk until the pain develops, then restfor a few minutes. Carry on walking when the pain has eased. Keep this up for at least 30 minutes each day, and preferably for an hour a day. The pain is not damaging to the muscles.
Other exercises such as cycling and swimming will also help you to become fit and are good for the heart. However, these should be done inaddition to walking, as walking has been shown to be the best exercise to improve symptoms of PAD.
Research studies have shown that if you stop smoking and exercise regularly, then symptoms of PAD are unlikely to become worse, and theyoften improve. Your risk of developing heart disease or a stroke will also be reduced. Lose weight if you are overweight Losing weight reduces the demands on the heart and leg muscles and reduces the risk of forming atheroma. You should eat a healthy diet This is the same as advised to prevent heart disease. This reduces the chance of atheroma forming. A practice nurse may advise you on how to eat a healthy diet. Also, see separate leaflet in this series, called 'Healthy Eating', for further details.
Five portions, and ideally 7-9 portions, of a variety of fruit and vegetables per day.
You should not eat much fatty food such as fatty meats, cheeses, full-cream milk, fried food, butter, etc. Ideally, you should use low-fat,mono-unsaturated or polyunsaturated spreads.
Try to include 2-3 portions of fish per week, at least one of which should be 'oily' (such as herring, mackerel, sardines, kippers, salmon,or fresh tuna).
If you eat meat, it is best to eat lean red meat or poultry such as chicken.
If you do fry, choose a vegetable oil such as sunflower, rapeseed or olive.
Try not to add salt to food and limit foods which are salty. Alcohol Some research suggests that drinking a small amount of alcohol helps to reduce the risk of developing cardiovascular diseases such as PAD. The exact amount is not clear, but it is a small amount. So, do not exceed the recommended amount of alcohol as more than the recommended upper limits can be harmful. That is, men should drink no more than 21 units of alcohol per week, no more than four units in any one day, and have at least two alcohol-free days a week. Women should drink no more than 14 units of alcohol per week, no more than three units in any one day, and have at least two alcohol-free days a week. Pregnant women should not drink at all. One unit is in about half a pint of normal strength beer, or two thirds of a small glass of wine, or one small pub measure of spirits. Take care of your feet Try not to injure your feet. Injury may lead to an ulcer or infection developing more easily if the blood supply to your feet is reduced. Do not wear tight shoes or socks which may reduce blood supply. Tell your doctor if you have any foot injury, pain in a foot when you are resting, or any marked change in skin colour or temperature in either of your feet. What are the treatments for peripheral arterial disease? The self-help measures above are the most important part of treatment. In addition, medication is often advised. Surgery is only needed in a small number of cases. Medicines Aspirin is usually advised. A daily low dose (75 mg) is usual. This does not help with symptoms of PAD, but helps to prevent blood clots (thrombosis) forming in arteries. It does this by reducing the stickiness of platelets in the blood stream. (Aspirin is an antiplatelet medicine.) A blood clot is an uncommon complication of PAD. However, as mentioned, people with PAD have a higher-than-average risk of developing a heart attack or stroke (which are usually caused by blood clots). A daily low dose of aspirin reduces this risk too. If you cannot take aspirin then alternative antiplatelet medicines such as clopidogrel and dipyridamole may be advised. A statin medicine is usually advised to lower your cholesterol level. This helps to prevent a build-up of atheroma. If you have diabetes then good control of your blood glucose level will help to prevent PAD from worsening. If you have high blood pressure then you will normally be advised to take medication to lower it. Other medicines are sometimes used to try to open up the arteries. For example, cilostazol and naftidrofuryl. One may be given and may help. However, they do not work in all cases. Therefore, there is no point in continuing with these medicines if you do not notice an improvement in symptoms within a few weeks. Surgery Most people with PAD do not need surgery. Your GP may refer you to a surgeon if symptoms of PAD become severe, particularly if you have pain when you are resting. Surgery is considered a last resort. There are three main types of operation for PAD: Angioplasty is where a tiny balloon is inserted into the artery and blown up at the section that is narrowed. This widens the affected segment of artery. This is only suitable if a short segment of artery is narrowed. Bypass surgery is where a graft (like a flexible pipe) is connected to the artery above and below a narrowed section. The blood is then diverted around the narrowed section. Amputation of a foot, or lower leg, is needed in an extremely small number of cases. It is needed when severe PAD develops and a foot becomes gangrenous due to a very poor blood supply. Further help and information The Circulation Foundation Web: Publishes a number of patient information leaflets to help identify and treat vascular illness. It also funds research into the prevention and causes of vascular disease. British Heart Foundation Greater London House, 180 Hampstead Road, London, NW1 7AW Tel (Heart Help Line): 0300 330 3311 Web: References
Diagnosis and Treatment of Peripheral Artery Diseases, European Society of Cardiology (2011)
Vascular disease - clopidogrel and dipyridamole, NICE Technology Appraisal Guideline (December 2010); Clopidogrel andmodified-release dipyridamole for the prevention of occlusive vascular events
Peripheral arterial disease - cilostazol, naftidrofyryl oxalate, pentoxifylline and inositol nicotinate, NICE Technology Appraisal Guideline(May 2011); Cilostazol, naftidrofyryl oxalate, pentoxifylline and inositol nicotinate for the treatment of intermittent claudication in peoplewith peripheral arterial disease
Diagnosis and management of peripheral arterial disease, Scottish Intercollegiate Guidelines Network - SIGN (2006)
Watson L, Ellis B, Leng GC; Exercise for intermittent claudication. Cochrane Database Syst Rev. 2008 Oct 8;(4):CD000990. [abstract]
Mazari FA, Gulati S, Rahman MN, et al; Early outcomes from a randomized, controlled trial of supervised exercise, Ann Vasc Surg. 2010Jan;24(1):69-79. Epub 2009 Sep 17. [abstract]
Robless P, Mikhailidis DP, Stansby GP; Cilostazol for peripheral arterial disease. Cochrane Database Syst Rev. 2008 Jan23;(1):CD003748. [abstract]
The evidence base for alcohol guidelines, Royal College of Physicians (2011)
Disclaimer: This article is for information only and should not be used for the diagnosis or treatment of medical conditions. EMIS has used allreasonable care in compiling the information but make no warranty as to its accuracy. Consult a doctor or other health care professional fordiagnosis and treatment of medical conditions. For details see our conditions. The clinicians responsible for the production of this document are:
Patie nt Inform ation
Copyright ĂŁ 2013, Egton Medical Information Systems Limited
The content prov ided in this leaf let is f or inf ormation purposes only . It is not designed to diagnose or treat a condition or otherwise prov ide medical adv ice. Inf ormation contained in thisleaf let is also subject to personal interpretation and can become obsolete, thus accuracy cannot be guaranteed. Please consult y our own healthcare prov ider regarding any medicalissues. Copyright 2013, DXS Ltd. All Rights Reserved
Andrea’s Help Sheet on Preparing Solutions There are several types of stock solutions made in the research lab: Percent (%) solutions, Molar (M) solutions, X solutions, and mg/ml solutions. First are instructions on how to make % solutions. First, know the definition of a % solution: 1% = 1g/100ml That’s the basic formula, and it is logical because “per cent” means “per hundredâ
medical education case study Management of chronic pelvic pain This case of persistent pelvic pain illustrates the multifactorial nature of the condition. By Mr Philip Kaloo well as the probable findings (recurrent endometriosis and case study pelvic adhesions) and the risk of complications. Laparoscopy Miss aP, a 28-year-old nulliparous woman, presented to the showed significant

 11 Jul 2012
11 Jul 2012