Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Www2.imm.dtu.dk
Arch Dis Child 1999;80:241–247
Systemic availability and pharmacokinetics ofnebulised budesonide in preschool children
L Agertoft, A Andersen, E Weibull, S Pedersen
Abstract
patient to patient, the average daily nominal
Aim—To evaluate the systemic availability
dose being 1 mg.2 3 Considering the ages and
and basic pharmacokinetic parameters of
body weights of preschool children, such a dose
budesonide after nebulisation and intra-
seems quite high compared with the recom-
venous administration in preschool chil-
mendations for adults and the dose required
dren with chronic asthma.
when a pressurised metered dose inhaler with a
Methods—Plasma concentrations budesonide measured
budesonide. For these reasons some paediatri-
hours after an intravenous infusion of
cians have raised safety concerns about neb-
125 µg budesonide. The children then
ulised budesonide treatment. However, be-
inhaled a nominal dose of 1 mg budeso- nide through the mouthpiece of a Pari LC
adults in airway calibre and anatomy of the
Jet Plus nebuliser connected to a Pari
upper airways, the inspiratory air flow dynam-
Master compressor, and the plasma con-
ics of children might be quite diVerent from
centrations of budesonide were measured
those of adults. Therefore, conclusions from
for another six hours. The amount of budesonide inhaled by the patient (“dose
systemic bioavailability of inhaled budesonide
to subject”) was determined by subtract-
should be extrapolated to young children with
ing from the amount of budesonide put
great caution. Indeed, nothing is known about
into the nebuliser, the amount remaining
the pharmacokinetics of budesonide in pre-
in the nebuliser after nebulisation, the
school children or the percentage of the nomi-
amount emitted to the ambient air (filter),
nal dose that becomes systemically available
and the amount found in the mouth rinsing water.
The aim of our study was to assess the abso-
Results—Ten patients aged 3 to 6 years
lute systemic availability and basic pharma-
completed both the intravenous and the
cokinetic parameters of budesonide given as a
inhaled treatment. The mean dose to sub-
nebulised suspension in young children via a
ject was 23% of the nominal dose. The sys-
widely used jet nebuliser, Pari LC Jet Plus con-
availability budesonide estimated to be 6.1% of the nominal dose
GmbH, Starnberg, Germany). In addition, the
(95% confidence intervals (CI), 4.6% to
method of assessing inhaled dose and nebuliser
8.1%) or 26.3% of the dose to subject (95%
output in vivo by inserting filters to the
CI, 20.3% to 34.1%). Budesonide clearance
inspiratory and expiratory outlets was evalu-
was 0.54 l/min (95% CI, 0.46 to 0.62), steady state volume of distribution 55 li- tres (95% CI, 45 to 68), and the terminal Patients and methods half life was 2.3 hours (95% CI, 2.0 to 2.6).
Children aged 3 to 6 years with chronic asthma
Conclusions—Approximately 6% of the nominal dose (26% of the dose to subject)
budesonide from a pressurised metered dose
reached the systemic circulation of young
inhaler with a spacer were included in the
children after inhalation of nebulised
study. All patients had to demonstrate a correct
budesonide. This is about half the sys-
inhalation technique with the Pari LC Jet Plus
temic availability found in healthy adults
nebuliser equipped with a mouthpiece. The
using the same nebuliser.
study was performed in accordance with the
(Arch Dis Child 1999;80:241–247)
Declaration of Helsinki. Written and verbal
Department of Paediatrics, Kolding
parents of all children before any study related
Hospital, DK-6000 Kolding, Denmark
The design was an open, single centre, phar-
Inhaled corticosteroids are normally adminis-
macokinetic study consisting of three visits to
tered to preschool children by a pressurised
the clinic. Visits 1 and 2 were separated by one
metered dose inhaler plus a spacer with a valve
to two weeks and visits 2 and 3 by no more than
Astra Draco AB, PO
system or by a jet nebuliser. Only a few clinical
one week. Two treatments were given: an intra-
Box 34, S-221 00, Lund, Sweden
dose finding studies have been conducted with
venous infusion of budesonide and a single
budesonide delivered by nebuliser in these age
inhaled dose of nebulised budesonide, both at
groups.1 2 These studies found that the mini-
visit 3. A semi-simultaneous design was used—
mum eVective dose required to control the dis-
that is, the two administrations were given in a
fixed order with the inhaled dose given three
severe asthma symptoms varied markedly from
hours after the start of the infusion. Agertoft, Andersen, Weibull, Pedersen
The patients rinsed their mouths twice with
The patient was instructed and trained in the
10 ml tap water directly after nebulisation and
correct use of the nebuliser using placebo.
the rinsing water was collected for later analy-
Correct use was considered to be tidal breath-
sis for budesonide content. The budesonide
ing without any pauses or leakage around the
content in the intravenous solution, on the
mouthpiece. A nose clip was worn during the
expiratory filter, in the ampoule, in the
inhalation. When the child had a correct inha-
nebuliser, and in the mouth rinsing water was
lation technique, he/she was given a nebuliser
with a compressor and placebo for further
method. Rigorous precautions were taken to
training at home before the next visit.
avoid contamination of the plasma sampleswith budesonide from the nebulisation.
Blood samples (4–5 ml) were drawn before
The patient’s inhalation technique was checked
the start of infusion (0), at the end of infusion
(placebo). This was followed by an inhalation
with filters (filter inhalation): an unused Pari
minutes after the start of infusion and at 180
LC Jet Plus nebuliser connected to a Pari Mas-
minutes after the start of infusion (immediately
ter compressor was equipped with an inspira-
before inhalation). In addition, samples were
tory filter between the nebuliser and the
taken at the end of inhalation and at 20, 40, 80,
mouthpiece and an expiratory filter attached to
160, 240, 330, and 360 minutes after the start
the expiratory outlet. The amount of drug
of inhalation. The plasma samples were stored
deposited on the inspiratory filter is assumed to
frozen until analysis for budesonide content.
be a measure of the amount of drug inhaled by
The total sampling time was nine hours and the
the patient while the amount on the expiratory
total blood volume taken from each child was
filter is considered to be a measure of the
amount of drug emitted to the ambient air
Venflon inserted for intravenous administra-
tion, the absolute systemic availability of
suspension and the patient inhaled as de-
scribed under visit 1. Nebulisation time was
ever, the inhalation and subsequent blood
five minutes. The nebuliser was tapped gently
sampling could still be carried out.
during nebulisation and it was ensured that the
The plasma concentration of the sum of the
patient had a correct inhalation technique. The
nebuliser was weighed before and after charg-
determined by a liquid chromatography plus
ing and after nebulisation. The filters were
mass spectrometry method. The lower limit of
stored in dark plastic bags at room temperature
quantification was 0.025 nmol/l. The between
until analysis for budesonide content by a
assay coeYcient of variation (CV) in control
samples run in parallel with the study samples
At the end of the visit, the nebuliser was dis-
mantled, thoroughly washed with ethanol, left
to dry, and then reassembled, ready to be usedagain by the same patient at visit 3.
IN VITRO CHARACTERISTICS OF THE NEBULISERPari LC Jet Plus delivers a dose of budesonide,
measured in vitro with filters, of about 23% of
Inhaled budesonide was discontinued two days
before visit 3. On arrival at the clinic, indwell-
0.5 mg/ml of budesonide. The droplet size,
ing catheters (Venflon; Becton Dickinson BOC
Malvern Mastersizer X (Malvern, Worcester-
serted in both arms after pretreatment with
shire, UK), is 5 µm. When charged with 2 ml of
budesonide suspension, the nebuliser normally
Södertälje, Sweden). One arm was used for
runs to dryness within five minutes.
intravenous infusion of budesonide and theother for blood sampling.
A budesonide solution (20 ml of 6.25 µg/ml,
total dose 125 µg) was infused manually at a
The dose inhaled by the patient during nebuli-
constant rate over 10 minutes. The infusion
sation was assessed at visits 2 and 3.
was followed by an injection of 5 ml sterilesaline to rinse the catheter before it wasremoved. A sample of the infused budesonide
solution was frozen for later analysis of
The amount of budesonide recovered from the
budesonide concentration. The syringe was
inspiratory (I) and expiratory (E) filters was
weighed before and after infusion to obtain the
used to estimate the inhaled dose, the total
output from the nebuliser (I + E), and the
measured concentration and the density of the
inhaled dose in percentage of the total output
infused solution, was used to calculate the
Three hours after the start of the infusion,
The “dose to subject” was calculated by
exactly the same way as during filter inhalation
subtracting from the assayed batch dose the
at visit 2, except that an inspiratory filter was
sum of the amounts of budesonide recovered
not used and the nebuliser was not weighed. Nebulised budesonide in preschool childrenMeasurement of inhaled budesonide dose, budesonide dose on expiratory filter, and inhaled dose in % of totaloutput in 12 preschool children by two diVerent methods (filter and drug inhalation)
G mean; geometric mean; CV, coeYcient of variation.
expiratory filter, the nebuliser with mouthpiece
ject), and F (systemic bioavailability after inha-
and connecting tubes, and the mouth rinsing
lation in percentage of nominal dose).
In the secondary analysis, the last observable
The inhaled dose was calculated as the sum
phase after the intravenous administration was
of the dose to subject and the amount of drug
assumed to be the terminal elimination phase
recovered from the mouth rinsing water.
after an intravenous dose (diVerent half lives)
The total output from the nebuliser was cal-
culated as dose to subject plus the amounts of
assumption. This may be interpreted as an
budesonide recovered from the mouth rinsing
absorption rate limited elimination for neb-
ulised budesonide (a flip flop phenomenon).
Doses and ratios between doses or amounts
This analysis might also provide an upper limit
from filter and drug inhalations were described
for the systemic availability if there is no flip
with the geometric mean and 95% confidence
flop, but the terminal phase after intravenous
limits using the t distribution. The nominal
administration starts later than three hours
dose was defined as the dose written on the
PARAMETRIC PHARMACOKINETIC ANALYSISA pharmacokinetic model was fitted to the
NON-PARAMETRIC PHARMACOKINETIC ANALYSESBecause the half life of the last observable
plasma concentration data using a non-linear
phase after intravenous administration was
mixed eVects model approach. The population
found to be shorter than the terminal half life
parameters were estimated using the Vonesh-
seen after inhalation, diVerent analyses based
Carter algorithm4 and approximate 95% confi-
were possible. In the primary analysis, the ter-
minal half life after intravenous administration
the intravenous administration because two
was assumed to be identical to the terminal half
clear phases were seen after the intravenous
life seen after inhalation (identical half lives).
dose and a third, slower phase, was seen after
Thus, the terminal elimination rate constant,
k was estimated from the plasma concentra-
tions after inhalation by mathematically fitting
a straight line to the last plasma measurements
included in our study. Ten patients completed
regression. The intravenous and the inhalation
both intravenous and inhaled treatment. One
curves were then separated from each other by
child received only inhaled treatment because
assuming that the terminal phase for the intra-
of problems with the intravenous administra-
venous dose was reached when the inhalation
tion. Two children were withdrawn because of
started, three hours after the intravenous dose.
lack of cooperation and problems with blood
sampling, but the inhalation data from one of
intravenous curve were subtracted from the
measured concentrations after inhalation to
children for comparison between filter and
drug inhalation. The mean age of the eight
The pharmacokinetic parameters calculated
budesonide administrations on visit 3 was 4.7
using non-parametric methods were described
years (range, 3–6). Their mean height was
with means and 95% confidence limits for the
109 cm (range, 95.5–121.0); mean weight was
mean calculated using the t distribution. Geo-
18.4 kg (range, 15.0–25.5). No adverse events
metric means were used for T1⁄ (terminal half
life), Cl (total clearance), V (volume of distri-
bution during terminal phase), V (volume of
A mean of 246 µg, or 25% of the nominal dose,
bioavailability in percentage of dose to sub-
was recovered from the inspiratory filter. This
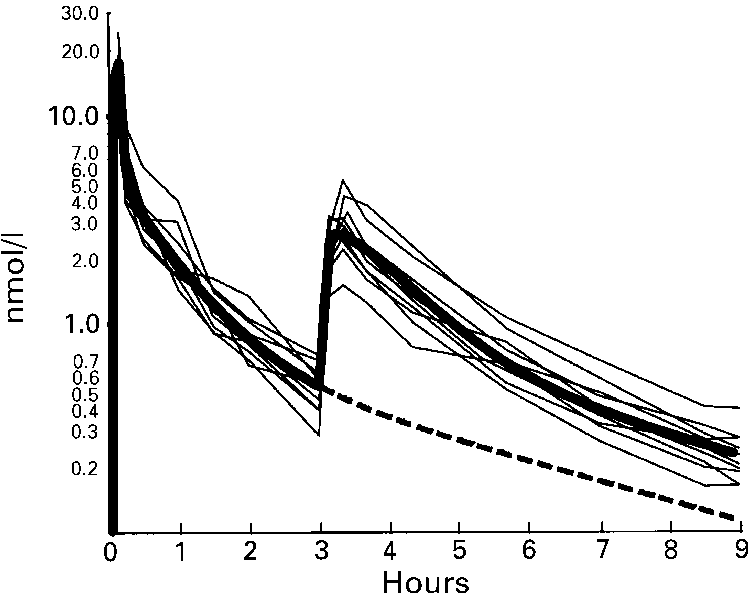
Agertoft, Andersen, Weibull, PedersenIndividual (thin lines) and estimated mean(bold and bold dashed lines) budesonide plasmaCorrelation between estimates of inhaled doseconcentration curves (log scale) in 10 preschool children(% of nominal) from filter inhalation and drug inhalationafter intravenous infusion of 117 µg budesonide andof budesonide from a Pari LC Jet Plus nebuliser in 12inhalation of 1000 µg budesonide from a Pari LC Jet Plusnebuliser. Mean curve was obtained from the parametricanalysis with a three exponential model.
corresponds to 57% of the total nebuliser out-put, which was 428 µg, or 43% of the nominal
on the expiratory filter after filter inhalation.
dose. The between-patient variation in these
Thus, the lower total output after filter inhala-
tion was mainly a result of a lower amount on
the expiratory filter after this inhalation.
The total output from the nebuliser (inhaled
dose + drug on expiratory filter) was 471 µg, or
47% of the nominal dose. The mean inhaled
117 µg) and the dose to subject ranged from
dose (dose to subject + amount in mouth rins-
192 to 273 µg (geometric mean, 232 µg). All
ing water) was 236 µg or 24% of the nominal
plasma samples after drug administration had
dose (50% of total nebuliser output). The
concentrations above the limit of quantifica-
tion. The individual plasma profiles after the
nominal dose). The between patient variation
consistent in shape (fig 2). The half life of the
magnitude as for the corresponding estimates
last observable phase after intravenous admin-
from the filter inhalation (table 1).
istration was shorter than the terminal half lifeseen after inhalation for all patients.
parameters and 95% confidence limits calcu-
In general, there was good agreement between
lated from the primary and secondary non-
the methods of assessing the inhaled dose dur-
parametric analyses and from the three expo-
ing nebulisation (table 1; fig 1). The mean ratio
between the amount on the inspiratory filter
availability in percentage of nominal dose or
and inhaled dose after drug inhalation was
percentage of dose to subject were very similar
in the three analyses, whereas half lives and
volumes of distribution were, as expected,
nebuliser after filter and drug inhalation was
somewhat lower in the non-parametric analysis
significantly lower total output after filter inha-lation. The mean ratio between the amounts
found on the expiratory filters after filter and
To enable comparison of clearance and vol-
umes of distribution with the values obtained
84%); there was a significantly lower amount
in adults in a previous study,5 these parameters
Estimated pharmacokinetic parameters of budesonide in 10 preschool children by: a non-parametric evaluationassuming identical terminal half lives after intravenous administration and inhalation; a non-parametric evaluationassuming diVerent terminal half lives after intravenous administration and inhalation; and by a three exponential model
Cl, total clearance; V , volume of distribution in terminal phase; V , volume of distribution at steady state; F
ability in % of dose to subject; F, systemic bioavailability in % of nominal dose. Nebulised budesonide in preschool childrenScaled pharmacokinetic parameters of budesonide in 10 preschool childrenestimated in a non-parametric evaluation assuming identical or diVerent terminal half livesafter intravenous infusion and inhalation of budesonideKey messages
reaches the systemic circulation of young
children after inhalation from a Pari LCJet Plus nebuliser
Cl, total clearance; V , volume of distribution in terminal phase; V , volume of distribution at
were expressed per kg body weight (table 3). In
addition, clearance was scaled to a 70 kg
subject by using weight0.75 as an adjustment
+ The low systemic availability in combina-
factor instead of simply scaling by weight1.0, 6.
Volumes were scaled to a 70 kg subject by
weight1.0 only. Table 3 gives a summary of the
parametric analysis, assuming identical termi-
nal half lives after infusion and inhalation. In
addition, the parameters from non-parametric
analysis assuming diVerent terminal half lives
after intravenous administration and inhalation
are given for comparison. No age dependence
+ A filter inhalation accurately assesses the
parameters or inhaled dose, as assessed by
individual patient it is only a crudesurrogate marker of the systemic avail-ability and dose of budesonide deposited
Discussion Our study provided important information
about the systemic availability of budesonide inyoung children after nebulisation. A systemicavailability around 6% is about half the value
previously found in healthy adults using the
deposited in the intrapulmonary airways by
personal communication, 1996) or with a Spira
inhalation.8 10 Therefore, the estimate of lung
synchroniser (15%).7 If the systemic availability
deposition in our study is probably close to the
is related to the dose to subject instead, the dif-
maximum achievable with the nebuliser used.
ference between children and adults seems
The use of a face mask is likely to reduce the
even more pronounced: 26% in children and
therapeutic ratio (clinical eVect/systemic eVect
ratio), whereas its influence on the total
niser) in adults. Lung deposition could be esti-
mated to be around 18% of dose to subject in
our children. This should be compared with
between the various pharmacokinetic param-
estimated lung depositions of 58% (synchro-
eters or inhaled dose and age, perhaps because
niser) and 70% (no synchroniser) in the two
the age range was too narrow. No other studies
adult studies. Furthermore, the deposition in
have assessed the possible age dependency of
the oropharynx was estimated to be ∼82% of
the various pharmacokinetic parameters of
dose to subject in young children compared
dependent lung deposition or drug delivery to
synchroniser) in adults. This indicates a very
the patient with various inhalation devices,11 12
diVerent deposition pattern in young children
whereas others have found lung deposition to
and adults, which is probably caused by the
smaller dimensions of the oropharynx and lar-
ynx in young children. These findings empha-
budesonide in children are sparse, so it is diY-
sise that conclusions from adult deposition
cult to make direct comparisons of our data
studies cannot be extrapolated to children. The
with the findings of others. In our study, mean
studies must be conducted in the age groups in
clearance was estimated to be around 30 ml/
which the inhaler is going to be used.
min/kg, which is ∼50% higher than in healthy
adults.5 This is in agreement with the findings
results are discussed it must be remembered
in older children.13 Volume of distribution/kg
that the standardised and very controlled study
body weight in steady state was about 15%
conditions diVered greatly from the day to day
higher than in adults,5 whereas the terminal
clinical treatment situation. In day to day treat-
half life after inhalation (2.3 hours) seemed to
ment, the variability in inhaled dose is likely to
be within the range of the terminal half life after
be higher and the lung deposition lower.8 9 In
intravenous administration in adults. In con-
these age groups, use of a face mask is often
trast, the half life after intravenous administra-
associated with inhalation through the nose,
tion (1.2 hours) was much shorter than in
Agertoft, Andersen, Weibull, Pedersen
adults. This could be a result of the study
size. Thus, these results do not support scaling
of the dose in mg/kg to limit systemic eVects.
followed for only three hours, and thus might
Nebulisation time was fixed to five minutes
have been truncated before the terminal phase
because in vitro tests before the study showed
was entered. These findings emphasise that
this to be long enough to run the nebulisers to
comparisons between studies with diVerent
dryness. A fixed time end point also avoided
sampling times and designs should be made
the diYcult judgment of “dryness” from the
with caution, because the results may vary with
sputtering sound of the nebuliser. In our study,
70% of the charged weight was lost during
A semi-simultaneous design was preferred to
nebulisation, suggesting that a nebulisation
administrations on separate days because of the
time of five minutes is suYcient to run the
reduction in intra-individual variation,14 a
nebulisers to dryness in vivo when a 2 ml
lower number of vein punctures, fewer blood
charge is used. Therefore, we do not believe
samples, a shorter sampling period, and an
that this aVected the conclusions of the study.
Filter studies are often used as surrogates for
measurable plasma concentrations. It has been
determination of the inhaled dose and lung
shown previously that the systemic availability
deposition of drug.11 12 16–19 However, the filter
of terbutaline could be estimated as accurately
method has not yet been validated in young
and precisely with this method as with the
children with asthma. In our study, there was
stable isotope method.15 In our study, however,
excellent agreement between the two ways of
the diVerent half lives seen after intravenous
assessing the inhaled dose. This is in accord-
administration and inhalation made several
ance with the results of a study in adults
interpretations possible. Either the terminal
assessing deposition of radiolabelled pentami-
half lives after intravenous administration and
dine in the intrapulmonary airways.20 21 How-
inhalation are identical and the intravenous
ever, the poor correlation between inhaled dose
curve is truncated before entering the terminal
and systemic availability in our study indicates
phase, or there is a diVerence in half lives as a
that important factors other than inhaled dose
result of an absorption rate limited elimination
influence the deposition of nebulised budeso-
of inhaled drug. An absorption rate limited
nide in the intrapulmonary airways. Our study
elimination of inhaled budesonide was consid-
does not allow any conclusion about which
ered an unlikely explanation for the diVerence
in half lives, because no such observations have
The amount of drug on the expiratory filter
been made in adult pharmacokinetic studies
and total drug output were slightly lower for
with Turbuhaler or pressurised metered dose
the filter inhalation compared with the drug
inhalers.5 However, the estimates of systemic
inhalation. The only diVerence between the
availability and clearance from all three diVer-
two experimental set ups was the absence of an
inspiratory filter during drug inhalation, sug-
mean availabilities in the range of 6–8% and
gesting that the introduction of an inspiratory
filter might have caused the diVerence. This
suggests that our conclusions are reasonably
suggestion is in accordance with the findings of
robust and not heavily dependent upon the
other studies.3 16 22 23 The reason for this change
is not clear. It might be a result of the increased
Young children often use nebulised doses of
dead space in the nebuliser or to the somewhat
budesonide that are in the same dose range as
higher resistance caused by the filter. This
those used by adults. This causes great concern
should be remembered when the findings of
among many paediatricians and it is often sug-
gested that nebulised drugs should be scaled toyoung children by dosing in mg/kg to reducethe risk of systemic side e
1 Ilangovan P, Pedersen S, Godfrey S, et al. Treatment of
severe steroid dependent preschool asthma with nebulised
budesonide suspension. Arch Dis Child 1993;68:356–9.
2 Wennergren G, Nordvall SL, Hedlin G, et al. Nebulized
budesonide for the treatment of moderate to severe asthma
in infants and toddlers. Acta Paediatr 1996;85:183–9.
The systemic exposure of drug measured as
3 Vikre-J¢rgensen J, Agertoft L, Pedersen S. Dose titration of
nebulized budesonide in young children. Pediatr Pulmonol
the area under the plasma concentration v time
1997;23:270–7.
curve (AUC) is normally thought to reflect the
4 Vonesh EF, Carter RL. Mixed eVect models for unbalanced
repeated measures. Biometrics 1992;48:1–18.
systemic activity of the treatment. Therefore, it
5 Thorsson L, Edsbäcker S, Conradson TB. Lung deposition
was interesting that the AUC/mg nominal dose
of budesonide from Turbuhaler is twice that from a pressu-rized metered dose inhaler (MDI).
in our study was very similar to the AUC/mg
Eur Respir J 1994;7:
nominal dose measured in adults using the
6 Holford N. A size standard for pharmacokinetics. Clin Phar-
same nebuliser (4.6 and 3.9 nmol/l × hour/mg,
macokinet 1996;30:329–32.
7 Dahlström K, Larsson P. Lung deposition and systemic
respectively) (E Bondesson, personal commu-
availability of budesonide inhaled as nebulised suspension
nication, 1996). The same was the case if the
from diVerent nebulisers. Journal of Aerosol Medicine 1995; 8:79.
calculation was done as AUC/mg dose to sub-
8 Chua HL, Collis GG, Newbury AM, et al. The influence of
ject (19.8 for children and 21.0 nmol/l ×
age on aerosol deposition in children with cystic fibrosis. Eur Respir J 1994;7:2185–91.
hour/mg for adults). This strongly suggests that
9 Mallol J, Rattray S, Walker G, et al. Aerosol deposition in
infants with cystic fibrosis. Pediatr Pulmonol 1996;21:276–
10 Everard ML, Hardy JG, Milner AD. Comparison of
nebuliser will be very similar in young children
nebulised aerosol deposition in the lungs of healthy adults following oral and nasal inhalation. Thorax 1993;48:1045–
and adults, despite the marked diVerence in
Nebulised budesonide in preschool children
11 Wildhaber JH, Devadason SG, Eber E, et al. Aerosol deliv-
17 Bisgaard H. Aerosol treatment of young children. Eur Respir
ery to wheezy infants: a comparison between a nebulizer
Rev 1994;4:15–20.
and two small volume spacers. Pediatr Pulmonol 1997;23:
18 Bisgaard H, Pedersen S, Nikander K. Use of budesonide
Turbuhaler in young children suspected of asthma. Eur
12 Devadason SG, Everard ML, MacErlan C, et al. Lung
Respir J 1994;7:740–2.
deposition from the Turbuhaler in children with cystic
19 Agertoft L, Pedersen S. Influence of spacer device on drug
fibrosis. Eur Respir J 1997;10:2023–8.
delivery to young children with asthma. Arch Dis Child
13 Pedersen S, SteVensen G, Ekman I, et al. Pharmacokinetics
1994;71:217–20.
of budesonide in children with asthma. Eur J Clin Pharma-
20 Smaldone GC. Deposition patterns of nebulised drugs: is
col 1987;31:579–82.
the pattern important? Journal of Aerosol Medicine 1994;
14 Karlsson MO, Bredberg U. Estimation of bioavailability on
7(suppl 1):S25–32.
a single occasion after semisimultaneous drug administra-
21 Smaldone GC, Fuhrer J, Steigbigel RT, et al. Factors deter-
tion. Pharmacol Res 1989;6:817–21.
mining pulmonary deposition of aerosolized pentamidine
15 Bredberg U, Karlsson MO, Borgström L. A comparison
in patients with human immunodeficiency virus infection.
between the semisimultaneous and the stable isotope tech-
Am Rev Respir Dis 1991;143:727–37.
niques for bioavailability estimation of terbutaline in
22 Everard ML, Clark AR, Milner AD. Drug delivery from
humans. Clin Pharmacol Ther 1992;52:239–48.
holding chambers with attached facemask. Arch Dis Child
16 Lödrup Carlsen KC, Nikander K, Carlsen KH. How much
1992;67:580–5.
nebulised budesonide reaches infants and toddlers? Arch
23 Agertoft L, Pedersen S. Importance of the inhalation device
Dis Child 1992;67:1077–9.
on the eVect of budesonide. Arch Dis Child 1993;69:130–3. Systemic availability and pharmacokinetics of nebulised budesonide in preschool children
L Agertoft, A Andersen, E Weibull, et al. Arch Dis Childdoi: 10.1136/adc.80.3.241
Updated information and services can be found at:
References
This article cites 20 articles, 10 of which can be accessed free at:
Email alerting
Receive free email alerts when new articles cite this article. Sign up in the
box at the top right corner of the online article.
Articles on similar topics can be found in the following collections
Collections
CURRICULUM VITAE __________________________________________________________________________________________ FULL NAME AND DEGREE/S: EDUCATION: Institution ACADEMIC APPOINTMENTS: 1995-1996 Research Assistant, M .S. Swaminathan Research Foundation, India 1996-1999 Teaching Assistant, School of Dietetics and Human Nutrition, McGill University, Canada 1999-2000 Res
V i s m e d i c a t r i x n a t u r a e FOOD MULTI II Rationale Disclaimer: The information within is for professional use only and is not intended as medical advice. The authors and Innate Response Formulas®, a division of BioSan Laboratories,disclaim any liability arising directly or indirectly from the use of the information within. Food Multi II Rationale Crafted as a foundationa
 Agertoft, Andersen, Weibull, Pedersen
Individual (thin lines) and estimated mean
(bold and bold dashed lines) budesonide plasma
Correlation between estimates of inhaled dose
concentration curves (log scale) in 10 preschool children
(% of nominal) from filter inhalation and drug inhalation
after intravenous infusion of 117 µg budesonide and
of budesonide from a Pari LC Jet Plus nebuliser in 12
inhalation of 1000 µg budesonide from a Pari LC Jet Plus
nebuliser. Mean curve was obtained from the parametricanalysis with a three exponential model.
corresponds to 57% of the total nebuliser out-put, which was 428 µg, or 43% of the nominal
on the expiratory filter after filter inhalation.
Agertoft, Andersen, Weibull, Pedersen
Individual (thin lines) and estimated mean
(bold and bold dashed lines) budesonide plasma
Correlation between estimates of inhaled dose
concentration curves (log scale) in 10 preschool children
(% of nominal) from filter inhalation and drug inhalation
after intravenous infusion of 117 µg budesonide and
of budesonide from a Pari LC Jet Plus nebuliser in 12
inhalation of 1000 µg budesonide from a Pari LC Jet Plus
nebuliser. Mean curve was obtained from the parametricanalysis with a three exponential model.
corresponds to 57% of the total nebuliser out-put, which was 428 µg, or 43% of the nominal
on the expiratory filter after filter inhalation. Systemic availability and pharmacokinetics of
Systemic availability and pharmacokinetics of