Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Use of this content is subject to the Terms and Conditions of the MD Consult web site.
Journal of the American Academy of Child and Adolescent Psychiatry Volume 44 • Number 4 • April 2005 Copyright 2005 Williams & Wilkins Articles An Open-Label Trial of Escitalopram in Pervasive Developmental Disorders
THOMAS OWLEY M.D. 1 LAURA WALTON R.N., M.ED 1 JEFF SALT D.CLIN.PSY 1 STEPHEN J. GUTER JR M.A. 1 MARREA WINNEGA PH.D. 1 BENNETT L. LEVENTHAL M.D. 1 EDWIN H. COOK JR M.D. 1 1 All authors are with the Department of Psychiatry, University of Chicago. Accepted November 11, 2004. This study was funded by National Institute of Health grants KOI MH64539 (T.O.)and U19HD35482(E.H.C). The authors also acknowledge the generous support of the Jean Young and Walden W. Shaw Foundation and the University of Chicago General Clinical Research Center (NIH grant M01 RR00055).Correspondence to Dr. Thomas Owley, Department of Psychiatry, University of Chicago, MC 3077, 5841 South Maryland Avenue, Chicago, IL 60637; e-mail: towley@yoda.bsd.uchicago.edu. 0
2005 by the American Academy of Child and Adolescent Psychiatry.
ABSTRACT Objective: To assess the effect of escitalopram in the treatment of pervasive developmental disorders (PDDs). Method: This 10-week study had a forced titration, open-label design. Twenty-eight subjects (mean age 125.1 ± 33.5 months) with a PDD received escitalopram at a dose that increased weekly to a maximum dose of 20 mg as tolerated. The Aberrant Behavior Checklist-Community Version (ABC -CV) and the Clinical Global Impression scale (CGI) were used to assess outcome. Results: There was significant improvement in ABC-CV Irritability Subscale Scores (baseline mean 20.5 ± 5.9 to final mean 10.9 ± 7.2; p < .001) and in the other ABC-CV Subscales. Improvement on Clinical Global Improvement Scale severity rating was also significant (baseline mean 5.2 ± 1.0 to final mean 4.6 ± 1.2; p < .001). Twenty-five percent of the subjects responded at a dose less than 10 mg and did not tolerate the 10-mg dose, and an additional 36% responded at a dose greater than or equal to 10 mg. Final dose was unrelated to weight and only weakly correlated with age. Conclusions: This open-label study found escitalopram to be useful in treating some difficulties common in PDDs. A wide variability in dose was found that could not be accounted for by weight and only partially by age. The study provides information useful for the design of double-blind, placebo -controlled studies of escitalopram in PDDs. J. Am. Acad. Child Adolesc. Psychiatry, 2005;44(4):343–348.
http://home.mdconsult.com/das/article/body/47251345-2/jorg=journal&source=MI&sp=15395743&sid=0. 5/16/2005
Key Words:
autistic disorder escitalopram drug treatment open label
The pervasive developmental disorders (PDDs) are a group of debilitating neurodevelopmental disorders characterized by qualitative Impairment in reciprocal social behavior, language and communication, and restrictive, repetitive, and stereotyped behaviors and interests (American Psychiatric Association, 1994) . Traditionally, medications nave been used to address symptoms of the disorder such as anxiety, obsessions/compulsions, hyperactivity, mood disturbances, and aggression (Owley, 2002) .
Potent serotonin transporter inhibitors are often used to address symptoms of compulsions or repetitive behaviors, obsessions, anxiety/irritability, and depression. Potent serotonin transporter inhibitors include the selective serotonin reuptake inhibitors (SSRIs) fluoxetine, sertraline, paroxetine, fluvoxamine, citalopram, and escitalopram as well as the less selective but comparably potent serotonin transporter inhibitor clomipramine, a tricyclic antidepressant. This group of medications appears to be most useful when insistence on routines or rituals are present to the point of manifest anxiety or aggression in response to interruption of the routines, preoccupations, or rituals ( Brodkin et al., 1997 ; Cook et al., 1992 ; Gordon et al., 1993 ) or with a comorbid disorder such as major depression, obsessive-compulsive disorder, and anxiety disorder ( Ghaziuddin et al., 1991 ; Kroenke et al., 2001 ).
Open-label investigations of the SSRIs have shown promise for these medications in the treatment of PDDs. In a sample that included adults and children with PDDs, a majority of subjects (15/23) responded favorably to fluoxetine (Cook et al., 1992) , and a similar response was found with sertraline (24/42 having a favorable response) in another open-label study of adults with PDDs (Hellings et al., 1996) . In a prospective, open-label trial of clomipramine in adults with PDDs, the medication was found to be helpful in decreasing obsessions, compulsions, and aggression (Brodkin et al., 1997) .
Controlled studies have also suggested the usefulness of potent serotonin transporter inhibitors in the treatment of some symptoms of PDDs. Gordon et al. (1993) found clomipramine to be superior to desipramine and placebo in improving some behavioral symptoms of PDDs. In a double-blind, placebo-controlled trial, fiuvoxamine was found to be helpful in about half of those adults receiving the medication and to be significantly more effective than placebo overall (McDougle et al., 1996) .
Despite the evidence of the usefulness of SSRIs in the treatment of many patients with PDDs, many questions about the use and dosing of these medications remain. It is not clear why some subjects have a positive response and others do not. Extensive clinical use of these agents also suggests that dosing these medications is not easy: For reasons that are poorly understood, this population shows a wide variability in dose response to this class of medications, with some patients being unable to tolerate very small doses of SSRIs before side effects emerge. The common side effects associated with SSRIs in this population, which appear to be dose related, are decreased appetite, irritability, motor restlessness, insomnia, and elation (Carlson and Mick, 2003) . The onset of irritability and/or early morning awakening or an increased latency in getting to sleep are particularly apt to occur when the dose is too high. It is possible that increased variability in dose-related onset of side effects as well as response is related to the well-replicated findings of serotonergic dysfunction in PDDs ( Cook and Leventhal, 1996 ; Schain and Freedman, 1961 ).
Clinical experience suggests that the typical course when SSRJ titration is undertaken is to see a decrease in anxiety and irritability until a particular threshold dose is reached, at which time dose-related side effects such as sleep
http://home.mdconsult.com/das/article/body/47251345-2/jorg=journal&source=MI&sp=15395743&sid=0. 5/16/2005
difficulties (latency to sleep and/or early morning awakening), elation, decreased appetite, motor restlessness, disinhibition, and increased irritability emerge (Owley, 2002) . At this time, it is best to reduce the medication to the highest previously tolerated dose. Because of the perceived sensitivity in those with PDDs to these agents, it is hypothesized that starting at a low dose and titrating slowly upward would prove superior in terms of outcome versus starting at a typical dose used in other disorders.
This report is of 28 consecutive subjects between 6 and 17 years of age who received an SSRI, escitalopram, in a prospective, open-label study in which the medication was given according to a forced titration.
Subjects
A sample of 28 subjects (25 males and 3 females) (Table 1) between the ages of 6 and 17 years of age (mean 125.1 ± 33.5 months) who fulfilled criteria for a FDD (20 subjects with an autistic disorder, 5 subjects with Asperger’s disorder, 3 subjects with FDD, not otherwise specified) by all three of the following: Autism Diagnostic Interview-Revised (ADI-R) (Lord et al., 1994) , Autism Diagnostic Observation Schedule (ADOS) (Lord et al., 2000) , and DSM-IV criteria used by a psychiatrist experienced in the diagnosis of PDDs (T.O.), The ADI-R is a comprehensive, investigator-based interview that covers most developmental and behavioral aspects of autism. It was administered to the subject’s primary caregiver. The ADOS is a standardized observation of social, communicative, and repetitive behavior that is performed directly with the child over a period of 30 to 40 minutes. It is organized into four overlapping modules according to the expressive language level of the subject. Both the ADI-R and the ADOS have a diagnostic algorithm keyed to DSM-IVl’ICD-10 criteria for the diagnosis of autistic spectrum disorders. Nonverbal IQ was obtained using the Raven’s Colored Progressive Matrices (Raven, 1947) or the nonverbal section of the Differential Abilities Scale (Elliott, 1990) .
TABLE 1 -- Demographic and Baseline Clinical Data
http://home.mdconsult.com/das/article/body/47251345-2/jorg=journal&source=MI&sp=15395743&sid=0. 5/16/2005
Note: NOS = not otherwise specified; ADI-R = Autism Diagnostic Inventory-Revised ( Lord et al., 1994 ); ADOS = Autism Diagnostic Observation Schedule ( Lord et al., 2000 ).
Subjects were included if the caregiver provided a score of 12 or higher on the Aberrant Behavior Checklist-Community Version Irritability Subscale (ABC-CV, described below (Aman et al., 1985) . This level of irritability was chosen because it was thought to be high enough to allow adequate change. Additionally, during week 0, before medication, a sleep diary was kept by the parents/caretakers that documented times asleep and awake (excessive variability in sleep would exclude the subject because an abrupt increase in sleep latency or early awakening were criteria used throughout the study to determine when the titrated dose was getting too high; a range in time of awakening of greater than 2 hours over 7 days would exclude the potential subject). All subjects were free of serious medical difficulties, including seizures, by medical history and physical examination. No subjects had previously been exposed to escitalopram, and all subjects were free of psychoactive medications for at least a month before beginning escitalopram (subjects previously on fluoxetine were free of this medication for at least 6 weeks).
After confirmation of a FDD by the above inclusion criteria and confirmation of a score of 12 or greater on the ABC-CV Irritability Subscale, the study and study drug were described in detail to the subjects and their parents. Informed consent was obtained from parents/caretakers of all subjects, and subjects provided assent when cognitive capacity allowed appropriate understanding. The University of Chicago Institutional Review Board approved this study. The described sample (N = 28) are the initial subjects treated as part of a larger study investigating the pharmacogenetics of the serotonin system in PDDs. Specifically, this sample and subsequent subjects (final N = 100) will undergo genetic analysis to see whether final dose and side effects are a function of variation in the serotonin transporter gene.
This was a 10-week open-label study. The dosing schedule followed forced titration, with weekly increasing doses of escitalopram (2.5, 5, 10, 15, and 20 mg) unless specific criteria for downward titration due to side effects were met. Lack of tolerability requiring Interruption of the forced titration was determined using two measures, a sleep diary and the ABC-CV. Specifically, significant change in sleep was operationalized as either (1) three consecutive days of an increase in time to get to sleep of 1 hour later than the average time to sleep during the baseline week or (2) three consecutive days of awakening of 1 hour earlier than the average time awakening during the baseline week. Either of these sleep problems would lead to a reduction of the dose to the highest previously tolerated dose. Significant increase in the ABC-CV Irritability or Hyperactivity Subscales (operationalized as an increase of greater than 10 points over the previous week on either scale) would also lead to a reduction in the dose to the highest previously tolerated dose. After a subject was dropped to the highest previously tolerated dose, the subject would remain on that dose for the remainder of the study.
http://home.mdconsult.com/das/article/body/47251345-2/jorg=journal&source=MI&sp=15395743&sid=0. 5/16/2005
Outcome Measures
The ABC-CV (Aman et al., 1985) was filled out weekly by parents/caretakers to determine response and help identify the onset of side effects. The ABC-CV is a 58-item questionnaire that was developed to identify the effects of medication and other rherapeutic interventions in those with developmental disorders and is scored from 0 (“not at all a problem”) to 3 (“problem is severe in degree”). It has an overall score and is also divided into five subscores (Irritability, Lethargy, Stereotypy, Hyperactivity, and Inappropriate Speech). It has been sensitive to drug effects in previous clinical trials of autistic disorder ( Jaselskis et al., 1992 ; King et al., 2001 ).
The Clinical Global Impression Scale (CGI) (National Institute of Mental Health, 1985) was completed at baseline, and at the end of weeks 4 and 10. The CGI is a seven-point investigator-completed scale that separately assesses both the severity of the disorder in each subject (from “normal ” to “extremely ill”) and the global improvement or change in response to medication of each subject (from “very much improved” to “very much worse”).
Data Analysis
Paired t tests of ABC-CV subscale scores and CGI ratings of overall clinical severity were performed for baseline versus end of week 10. As noted above, clinical experience has suggested that some children with PDDs are sensitive to very low doses of SSRIs; therefore, an additional responder analysis was undertaken to determine the percentage of responders who could not tolerate a 10-mg dose and the percentage of responders who tolerated 10 mg or more. Analysis was also undertaken to see whether the final dose correlated with age or weight using Pearson’s r.
Thirty-three subjects were assessed for participation in the study. Three subjects were excluded from the study when it was determined that the subjects were below the necessary inclusion score on the ABC-CV Irritability Subscale. Two subjects were excluded by ADI/ADOS testing (not thought to have a FDD after testing). Twenty-three of 28 subjects were able to finish the 10 weeks of the study. The other five subjects did not finish the study for various reasons. Two had a good response to escitalopram but were determined to have considerable continuing hyperactivity that required stimulant treatment in the context of significant school difficulties (additional medications were not allowed by the study protocol). One had no response to escitalopram and was having significant ongoing obsessions and compulsions that required adjunctive treatment with risperidone. Two had symptoms of disinhibition and aggression; one of these subjects had this response at the lowest dose (2.5 mg), and it remitted with discontinuation. The other subject had this response at 20 mg, but this disinhibition continued for some time even after complete discontinuation of escitalopram (this subject has subsequently had a good response to aripiprazole).
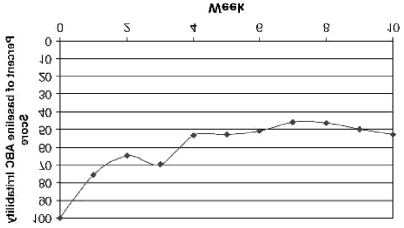
Paired t tests of ABC-CV outcome subscale scores and CGI severity ratings demonstrated improvement ( p < .001) (Table 2) . Improvement was noted in all the ABC-CV subscale scores (Irritability, Lethargy, Stereotypy, Hyperactivity, Inappropriate Speech). The percentage of baseline ABC-CV Irritability sub-scores by week is shown in Figure 1 . This figure shows a rapid and relatively regular drop in scores over the first 2 weeks that then levels off and plateaus around week 7.
TABLE 2 -- Effect of Treatment on Outcome Measures Measure/Subscale Mean ± SD Significance (p)
http://home.mdconsult.com/das/article/body/47251345-2/jorg=journal&source=MI&sp=15395743&sid=0. 5/16/2005
Note: ABC-CV = Aberrant Behavior Checklist, Community Version (Aman et al., 1985) ; CGI-S = Clinical Global Impression Scale (National Institute of Mental Health, 1985) .
*“0 mg ” refers to subjects who could not tolerate the 2.5-mg starting dose.
Figure 1. Percentage of baseline Aberrant Behavior Checklist (ABC)-Community Version Irritability scores by week.
http://home.mdconsult.com/das/article/body/47251345-2/jorg=journal&source=MI&sp=15395743&sid=0. 5/16/2005
With a decrease of 50% or more on the ABC-CV Irritability subscale score chosen a priori to define responders, 25% (7/28) of subjects responded at an optimal dose of less than 10 mg and could not tolerate the 10-mg dose and 36% (10/28) responded at and tolerated a dose greater than or equal to 10 mg. There was no significant relationship between final dose and weight (r = 0.181; p = .357), but there was a relatively weak correlation between final dose and age (r = 0.434; p= .021). There was no correlation between nonverbal IQ and ABC Irritability subscale scores (r = - 0.065; p= .758).
A substantial minority of responders (7/17 of responders and 10/28 treated subjects) could not tolerate a 10-mg dose. This sensitivity was best illustrated by a subject who previously had a reaction of extreme aggressiveness and insomnia when put on 10 mg paroxetine. Before this subject came to the study, he had subsequently been put on lithium and risperidone with some response but had side effects as well as continuing to have significant obsessions and compulsions. After he was tapered off his medications, he was titrated up to the 5-mg dose of escitalopram and had a reaction similar to that reported with paroxetine (but without insomnia). His dose was reduced to his highest previously tolerated dose (2.5 mg), at which he showed substantial improvement and was successfully continued on this monotherapy for more than 20 weeks since the end of his participation in the study.
DISCUSSION
This prospective, open-label study of escitalopram suggested that this medication is useful for the treatment of some symptoms of PDDs. The responder rate in this study (61%) is similar to that achieved in previous open-label studies of SSRIs in PDDs such as those of Brodkin et al. (1997) (55%), Cook et al. (1992) (65%), DeLong et al. (1998) (59%), and Hellings et al. (1996) (57%) and in placebo-controlled studies such as McDougle et al. (1996) (57%).
Of the subjects who finished the study (23), five individuals experienced no side effects and finished the study at the highest dose (20 mg). The other 18 subjects experienced dose-related side effects that required a reduction in dose to the previously highest tolerated dose. For seven subjects, this side effect was primarily irritability, for another six individuals, it was primarily hyperactivity, and for five subjects, high levels of both hyperactivity and irritability were noted. No subjects experienced suicidal ideation while taking escitalopram, and there was not any evidence of increased self-injurious behavior. It was expected that there -would be considerable sleep difficulties as a part of the side effect profile when subjects were titrated to a dose at which side effects emerged. Past experience with other SSRIs had indicated that sleep difficulties had been a reliable and often striking indicator of the dose being too high. With escitalopram, surprisingly, sleep changes were not present and did not lead to any dose changes in this study.
Clinical experience had suggested that there is wide variation in best final dose in this population. That was confirmed in this prospectively conducted open-label study. The mean final dose was 11.1 mg, with a wide SD of 6.5 mg and a range of 0 to 20 mg. As expected, there was no relationship between weight and final dose, suggesting that other factors are more relevant in determining a subject’s best dose. There was a weak correlation between age and final dose, accounting for 19% of the variance in final dose. Because the sample included pre- and postpubertal subjects, this may be an effect of pubertal physiological changes. Unfortunately, because no measure of sexual maturation was included in our protocol (i.e., Tanner stages), this question will require further study. The factors that are responsible for determining individual differences in tolerability and final dose are likely a combination of individual pharmacokinetic and pharmacodynamic differences.
Clinical Implications
The wide variability in the dose tolerated by subjects in this study, absence of correlation with weight, and weak correlation with age raises interesting clinical questions regarding the best approach to dosing in this population. There has long been evidence that, at least in this population, outcome is not related to the final dose of a potent serotonin reuptake-blocking agent. Gordon et al. (1993) found clomipramine to be very helpful in the treatment of 24 subjects with PDDs but found a 10-fold difference in plasma drug level that did not correlate individually or collectively with any clinical responses or adverse events. Again, in this study, we find no relationship between weight and final dose
http://home.mdconsult.com/das/article/body/47251345-2/jorg=journal&source=MI&sp=15395743&sid=0. 5/16/2005
tolerated. In this context, the prudent approach, and one that was effective here, would appear to start at a lower dose than usual and slowly increase while watching for the onset of side effects. In fact, clinical experience has shown that, in some cases, even a low dose is too much and that very small doses (e.g., 1 mg/day escitalopram elixir) may be necessary for some patients. This report is preliminary data from a larger study that hopes to answer some of these questions about dosing. The described sample and subsequent subjects will have genetic analyses done to see whether the final dose is a function of variation in the serotonin transporter gene.
For reasons that are not clear, escitalopram did not interfere with sleep in this study, and sleep data (in the form of sleep diaries) did not lead to any dose changes. Although this study did not use any other SSRI to test this directly, experience with other SSRIs suggests that these medications typically lead to sleep difficulties that are usually quite evident when the dose is above the patient’s threshold (Cook et al., 1992) . In this study, despite the onset of irritability, hyperactivity, and other evidence of the need to lower the dose, there were no qualitative complaints or quantitative evidence of sleep difficulties. If this characteristic of escitalopram is evident on further testing, it may provide an option for the clinician who has tried other SSRIs but encountered sleep difficulties before the onset of therapeutic effects. On the other hand, in the absence of regularly provided data like the ABC used here, it may also make it more difficult for the clinician to identify side effects and subsequently determine the ideal dose because irritability and other changes may be more subtle or confused with worsening of preexisting irritability than highly disordered sleep.
Although irritability was the primary outcome variable in this study, there were also significant findings in other symptom domains (Table 2) . For instance, hyperactivity improved significantly in this study; it is possible that much of this activity was related to anxiety and that reductions in anxiety resulted in a reduction in hyperactivity. It is not clear why there were perceived improvements in inappropriate speech, although other investigators have also observed improvement in speech with SSRIs (McDougle et al., 1996) .
Limitations
The primary limitation in drawing conclusions from this study is the open-label design. There is a well -documented history of expectancy effects in this population (King et al., 2001) . This may have been responsible for some symptom change overall, and particularly in areas where this medication would not usually be thought of as being helpful (for instance, inappropriate speech). Placebo-controlled studies will be useful in establishing the efficacy of SSRIs in prepubertal children.
Additionally, one must be cautious in extending the results of these data for those with Asperger’s disorder and FDD, not otherwise specified because these groups were in the minority in this study (18% and 10%, respectively) compared with the larger group with autistic disorder (71%).
Disclosure: Dr. Leventhal receives reseach support from Abbott, Eli Lilly, GlaxoSmithKline, Shire, Pfizer, and Forrest Laboratories; he is on the speaker’s bureaus of Eli Lilly, GlaxoSmithKline, Pfizer, and Bristol-Meyers Squibb/Otsuka; and he has consulting relationships with Abbott, Eli Lilly, Janssen, McNeil, Pfizer, and GlaxoSmithKline. The other authors have no financial relationships to disclose.REFERENCES
1. Aman MG. Singh NN, Stewart AW, Field CJ (1985), The Aberrant Behavior Checklist: a behavior rating scale for the assessment of
treatment effects. Am J Ment Def 39:485 –491 2. American Psychiatric Association (1994), Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV). Washington, DC:
American Psychiatric Association Press 3. Brodkin ES, McDougle CJ, Naylor ST, Cohen DJ, Price LH (1997), Clomipramine in adults with pervasive developmental disorders: a
prospective open-label investigation. J Child Adolesc Psychopharmacol 7:109–121 4. Carlson GA, Mick E (2003), Drug -induced disinhibition in psychiatrically hospitalized children. J Child Adolesc Psychopharmacol 13:153 –
http://home.mdconsult.com/das/article/body/47251345-2/jorg=journal&source=MI&sp=15395743&sid=0. 5/16/2005
163 5. Cook E, Leventhal B (1996), The serotonin system in autism. Curr Opin Pedintr 8:348 –354 6. Cook E, Rowlett R, Jaselskis C, Leventhal B (1992), Fluoxetine treatment of patients with autism and mental retardation. J Am Acad Child Adolesc Psychiatry 31:739 –745 7. DeLong GR, Teague LA, McSwain Kamran M (1998), Effects of fluoxetine treatment in young children with idiopathic autism. Dev Med Child Neurol 40:551 –562 8. Elliott C (1990), DAS Handbook. San Antonio, TX: The Psychological Corporation. 9. Ghaziuddin M, Tsai L, Ghaziuddin N (1991), Fluoxetine in autism with depression. J Am Acad Child Adolesc Psychiatry 30:508 –509 10. Gordon C, State R, Nelson J, Hamburger S, Rapoport J (1993), A double-blind comparison of clomipramine, desipramine, and placebo in
the treatment of autistic disorder. Arch Gen Psychiatry 50:441 –447 11. Hellings JA, Kelley LA, Gabrielli WF, Kilgore E, Shah P (1996), Sertraline response in adults with mental retardation and autistic disorder.
J Clin Psychiatry 57:333 –336 12. Jaselskis CA, Cook EH, Fletcher KE, Leventhal BL (1992), Clonidine treatment of hyperactive and impulsive children with autistic
disorder. J Clin Psychopharmacol 12:322 –327 13. King B, Wright D, Handen B et al. (2001), A double -blind, placebo -controlled study of amantadine hydrochloride in the treatment of
children with autistic disorder. J Am Acad Child Adolesc Psychiatry 40: 658 –665 14. Kroenke K, West SL, Swindle R et al. (2001), Similar effectiveness of paroxetine, fluoxetine, and sertraline in primary care: a randomized
trial. JAMA 286:2947–2955 15. Lord C, Risi S, Lambrecht L et al. (2000), The autism diagnostic observation schedule -generic: a standard measure of social and
communication deficits associated with the spectrum of autism. J Autism Dev Disord 30:205 –223 16. Lord C, Rutter M, Le Couteur A (1994), Autism Diagnostic Interview -Revised: a revised version of a diagnostic interview for caregivers of
individuals with possible pervasive developmental disorders. J Autism Dev Disord 24:659 –685 17. McDougle C, Naylor S, Cohen D, Volkmar F, Heninger G, Price L (1996), A double -blind, placebo -controlled study of fluvoxamine in
adults with autistic disorder. Arch Gen Psychiatry 53:1001–1008 18. National Institute of Mental Health (1985), Special feature: rating scales and assessment instruments for use in pediatric
psychopharmacology research. Psychopharmacol Bull 21:839 19. Owley T (2002), The pharmacological treatment of autistic spectrum disorders. CNS Spectr 7:663 –669 20. Raven J (1947), Coloured Progressive Matrices. Oxford: Oxford Psychologists Press 21. Schain RJ, Freedman DX (1961), Studies on 5 -hydroxyindole metabolism in autistic and other mentally retarded children. J Pediatr 58:315 –
Copyright 2005 Elsevier Inc. All rights reserved.
Bookmark URL: /das/journal/view/47251345 -2/N/15395743?ja=463157&PAGE=1.html&ANCHOR=top&source=MI
http://home.mdconsult.com/das/article/body/47251345-2/jorg=journal&source=MI&sp=15395743&sid=0. 5/16/2005
NHS Series The first feature is the large moment load. The THK LM guide is used with two rails to withstand high moment load. The second feature is ample options. Full stroke adjustment (one or both sides), with cable bearer (horizontal or vertical), and other options to match piping port positions, etc., is selectable. The X axis module sensor is installed on the T groove on the front c
Netta OR Soprano Netta Or was born in Israel, she studied at the Music High School in Cologne with Prof. Leisenheimer and joined master classes of Kurt Moll and Joan Dorneman, already with ten years she sang smaller roles like 1° Knabe in „Zauberflöte“ and appeared in „Macbeth“ at the theatre of Aachen . First guest contracts brought her to the theatre in Bonn as Serpina in
 Note: ABC-CV = Aberrant Behavior Checklist, Community Version (Aman et al., 1985) ; CGI-S = Clinical Global Impression Scale (National Institute of Mental Health, 1985) .
Note: ABC-CV = Aberrant Behavior Checklist, Community Version (Aman et al., 1985) ; CGI-S = Clinical Global Impression Scale (National Institute of Mental Health, 1985) .