Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Layout
284jumonline.qxp:Layout 1 3/17/09 2:30 PM Page 541
Case Report Inspissated Bile Syndrome in a Neonate Treated With Cefotaxime
Sonographic Aid to Diagnosis, Management,and Follow-up
Tamir Miloh, MD, Henrietta Kotlus Rosenberg, MD,Israel Kochin, MD, Nanda Kerkar, MD
holelithiasis in neonates is usually pigmentary and composed of calciumbilirubinate.1,2 In children, cholelithisasis and inspissated bile or sludge areassociated with prematurity, cystic fibrosis, hemolytic diseases, hemorrhage,
Ccongenital heart disease, starvation, total parenteral nutrition, infection,
dehydration, ileal resection, abdominal surgery, congenital anomalies of the biliarytract, chronic liver disease, medications (ceftriaxone), and up to 43% of cases are idio-pathic.2,3 We report the case of a neonate who had recurrent cholestasis after beingtreated for sepsis with cefotaxime.
Case Report Abbreviations
This 5-lb 15-oz full-term female neonate had an uncom-
ALT, alanine aminotransferase; AST, aspartate amino-
plicated perinatal history, a normal vaginal delivery, and
transferase; CBD, common bile duct; GGT,
γ-glutamyltransferase; UDCA, ursodeoxycholic acid
normal newborn screening results. She was brought to alocal hospital at 2 weeks of age with fever, abdominal dis-tension, vomiting, jaundice, and acholic stools. Pertinentlaboratory results included normal electrolyte levels, an aspartate aminotransferase (AST) level of 131 IU/L, analanine aminotransferase (ALT) level of 41 IU/L, and an alkaline phosphatase level of 106 IU/L (all normal for
Received October 30, 2008, from the Departments
age). Abnormal laboratory values included a γ-glutamyl-
of Pediatrics (T.M., H.K.R., I.K.) and Radiology
transferase (GGT) level of 613 IU/L (normal value for age,
(H.K.R., N.K.), Mount Sinai Medical Center, NewYork, New York USA. Revision requested
<300 IU/L), total/direct bilirubin levels of 4.5/2.9 mg/dL
November 19, 2008. Revised manuscript accepted
(normal, <1.2/0.8 mg/dL), and a blood culture positive
Address correspondence to Tamir Miloh, MD,
for Aeromonas hydrophila and Klebsiella pneumoniae. Department of Pediatrics, Mount Sinai Medical
Initial sonography showed ascites with an unremarkable-
Center, 1 Gustave L. Levy Pl, New York, NY 10029
appearing liver and no evidence of intrahepatic or extra-
E-mail: tamir.miloh@mountsinai.org
hepatic biliary ductal ectasia or biliary sludge.
2009 by the American Institute of Ultrasound in Medicine • J Ultrasound Med 2009; 28:541–544 • 0278-4297/09/$3.50
284jumonline.qxp:Layout 1 3/17/09 2:30 PM Page 542
Inspissated Bile Syndrome in a Neonate Treated With Cefotaxime
The neonate was treated with intravenous ampi-
bin levels of 4.4/4.3 mg/dL. Sonography showed
cillin and cefotaxime for 10 days. Enteral feedings
a cholestatic pattern in the liver, dilatation of the
were resumed by the third hospital day. On dis-
intrahepatic and extrahepatic biliary ducts,
charge, the jaundice had resolved (bilirubin,
common bile duct (CBD) size of 5 mm, a fluid-
1/0.5mg/dL), and the liver enzymes declined to an
debris level in the extrahepatic biliary ducts
AST level of 38 IU/L, an ALT level of 18 IU/L, and
consistent with dependent sludge, and a large
sludge ball in the gallbladder, which contained
One week after discharge, jaundice and acholic
nonshadowing brightly echoic foci suspicious for
stools recurred without any associated symp-
cholelithiasis (Figure 1). She was given ursodeoxy-
toms, and she was referred to our institution.
cholic acid (UDCA) at a dose of 15 mg/kg twice a
Physical examination was unremarkable aside
day, fat-soluble vitamins, a medium-chain triglyc-
from mild hepatomegaly. Laboratory blood tests
eride-rich formula, and intravenous hydration.
revealed an AST level of 101 IU/L, an ALT level of
Her stools became pigmented after 2 days, and
33 IU/L, an alkaline phosphatase level of 250
subsequent abdominal sonography on the sixth
IU/L, a GGT level of 1197 IU/L, and total biliru-
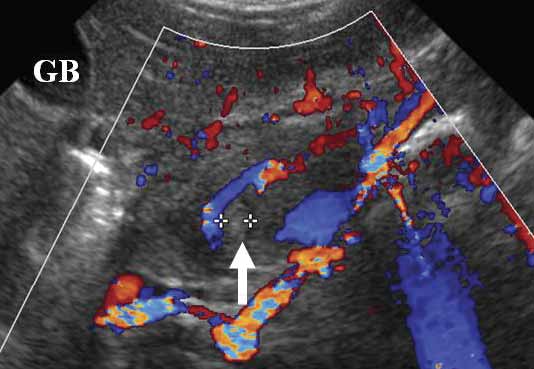
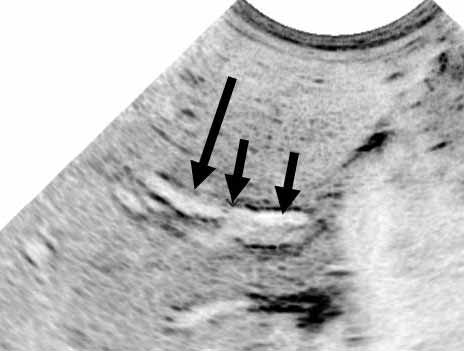
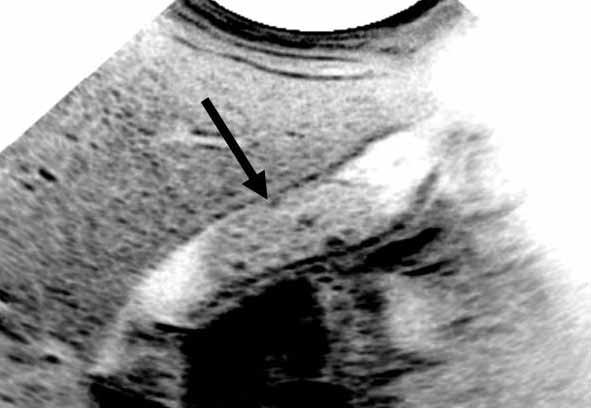
Figure 1. A, Sonogram of the dilated common hepatic duct (large arrow) and dilated CBD (small arrows) with a fluid-debris level noted within the distal CBD due to biliary sludge. The diameter of the CBD measured 0.5 cm. B, Color Doppler sonogram clearly dif- ferentiating between the dilated extrahepatic ducts and the surrounding vascular structures. Once again, sludge is noted within the distal CBD (arrow). C, Transverse sonogram in the region of the head of the pancreas showing brightly echoic sludge (arrow) filling the distal CBD at the level of the head of the pancreas. GB indicates gallbladder. D, Longitudinal sonogram of the gallbladder show- ing the presence of a large sludge ball (arrow) within the lumen, which contains several small focal nonshadowing more brightly echoic foci suspicious for precipitated material. The gallbladder is otherwise sonographically normal.
284jumonline.qxp:Layout 1 3/17/09 2:30 PM Page 543
Miloh et al
reduction in the size of the CBD to 3 mm. She
nosis of anatomic abnormalities that may cause
was discharged and continued to receive UDCA.
biliary obstruction and in most cases obviates
At 6 months of age, she was thriving; bilirubin
the need for higher-tech imaging studies and
levels were 0.2/0.1 mg/dL; transaminase levels
prevents unnecessary interventional procedures
were less than 50 IU/ml; and her GGT level was
23 IU/L (normal). Delayed sonography showed
The incidence of inspissated bile syndrome is 1
complete resolution of the biliary ductal dilata-
per 175,000 live births in England and accounts
for about 8% of all surgical jaundice duringinfancy.5 Biliary sludge appears sonographically
Discussion
as low-level echoes. On microscopy a mixture ofparticulate matter appears when various biliary
Early diagnosis of the underlying etiology of
solutes precipitate cholesterol, calcium bilirubi-
cholestasis in neonates is essential so that appro-
nate or other calcium salts, mucus, undefined
priate therapy can be promptly instituted. A
residues, and protein-lipid complexes. The diag-
direct bilirubin level of greater than 1 mg/dL (if
nosis of sludge is almost always based on imaging.
the total bilirubin level is <5 mg/dL) or greater
The pathogenesis of sludge is similar to that of
than 20% of the total bilirubin level (if the total
gallstones, which are formed from precipitating
bilirubin is level is >5 mg/dL) is diagnostic of
sludge.6 There are many predisposing factors to
conjugated hyperbilirubinemia. Jaundice, per-
the development of inspissated bile, sludge, or
sistent acholic stools, and an elevated GGT level
cholelithiasis in neonates.1–3 Ceftriaxone pseudo -
are suggestive of obstructive jaundice. In the
lithiasis, composed of precipitated ceftriaxone, is
neonatal period, the differential diagnosis of
reported to occur in 29.5% to 45.7% of children
obstructive cholestasis includes biliary atresia, a
treated with ceftriaxone.3 The pseudolithiasis
choledochal cyst, gallstones or biliary sludge,
occurs after 4 to 22 days (mean, 9 days) of ceftriax-
inspissated bile syndrome, cystic fibrosis, neona-
one therapy and resolves after 2 to 63 days (mean,
tal sclerosing cholangitis, and congenital hepatic
15 days) from the end of treatment.7 Cefotaxime, a
fibrosis/Caroli disease.4 Meticulous sonographic
third-generation cephalosporin, was previously
evaluation of the liver, spleen, pancreas, biliary
reported to be associated with pseudolithiasis in 2
ducts, and biliary vessels along with clinical and
of 34 infants (6%) who had cholelithisis.1 This
laboratory correlation allows for accurate diag-
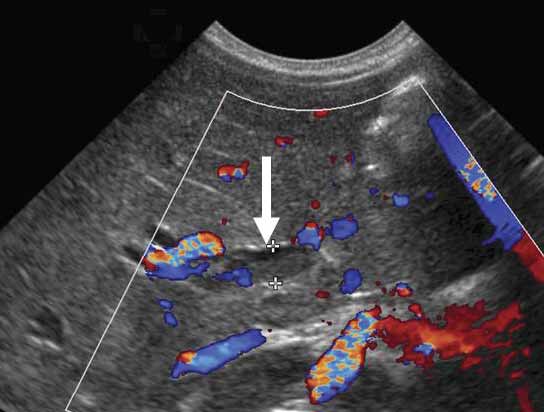
relationship was not found in 38 older childrenreceiving cefotaxime for 4 to 7 days.3 Therefore,this association may be unique in the neonatalpopulation. Figure 2. After treatment with UDCA, fat-soluble vitamins, and intravenous hydration, the neonate’s stools became pigmented
In most patients, removal of the precipitating
after 2 days, and subsequent abdominal sonography showed no
factor can lead to spontaneous resolution of bil-
evidence of intrahepatic or extrahepatic biliary ductal ectasia,
iary sludge. The refractory cases of inspissated
stones, sludge, or pericholecystic fluid.
bile syndrome and those associated with biliary-type pain, cholecystitis, cholangitis, or pancre-atitis are treated with open or laparoscopiccholecystectomy. Some may require endo-scopic retrograde cholangiopancreatographicsphincterotomy, percutaneous transhepaticcholangiographic saline flushing, or infusion ofN-acetylcysteine into the extrahepatic biliaryducts to prevent further episodes of cholangitisand pancreatitis.2 In asymptomatic patients, thesludge can be managed expectantly. Our patient’scholestasis resolved with hydration and high-dose (30-mg/kg/d) UDCA. Ursodeoxycholic acidis a hydrophilic bile acid that enriches the bile
284jumonline.qxp:Layout 1 3/17/09 2:30 PM Page 544
Inspissated Bile Syndrome in a Neonate Treated With Cefotaxime
acid pool, decreases the biliary saturation of
Keizman D, Ish-Shalom M, Konikoff FM. The clinical signif-
cholesterol, and may prevent sludge formation.8,9
icance of bile duct sludge: is it different from bile ductstones? Surg Endosc 2007; 21:769–773.
It was found to resolve symptoms in pediatricpatients with gallstones; however, the stones
Herek O, Pakdemirli E, Kocer N. Ceftriaxone-associated bil-iary pseudolithiasis in children. Eur Radiol 2001; 11:902.
transiently disappeared in only 2 of 15 patients inone study10 and in 8 of 180 in another.11
Jain R. Biliary sludge: when should it not be ignored? CurrTreat Options Gastroenterol 2004; 7:105–109.
The neonate we report was born full term, had
normal newborn screening results, and was not
Arslanoglu S, Moro GE, Tauschel HD, Boehm G. Ursodeoxycholic acid treatment in preterm infants: a pilot
dehydrated when she had inspissated bile syn-
study for the prevention of cholestasis associated with total
drome. The initial outside liver sonography dur-
parenteral nutrition. J Pediatr Gastroenterol Nutr 2008;
ing the septic period did not reveal sludge
despite biochemical cholestasis. Obstructive
Gamba PG, Zancan L, Midrio P, et al. Is there a place for
jaundice recurred 1 week after recovery from
medical treatment in children with gallstones? J Pediatr
sepsis. Because the neonate did not have any
other risk factors for development of inspissated
Della Corte C, Falchetti D, Nebbia G, et al. Management of
bile, the potential association was treatment with
cholelithiasis in Italian children: a national multicenterstudy. World J Gastroenterol 2008; 14:1383–1388.
cefotaxime, which may be unique in the neona-tal period.
In conclusion, obstructive jaundice in neonates,
as a consequence of inspissated bile or sludge,may follow treatment with cefotaxime and is like-ly to respond to hydration and medical manage-ment with UDCA. We emphasize the use ofsonography in the diagnosis, treatment, and fol-low-up of neonates with inspissated bile syn-drome, which in most cases obviates the need forhigher-tech imaging studies and prevents unnec-essary interventional procedures or surgery. The cholestasis and extrahepatic obstructionresolved with hydration and high-dose UDCA. References
Klar A, Branski D, Akerman Y, et al. Sludge ball, pseu-dolithiasis, cholelithiasis and choledocholithiasis fromintrauterine life to 2 years: a 13-year follow-up. J PediatrGastroenterol Nutr 2005; 40:477–480.
Debray D, Pariente D, Gauthier F, Myara A, Bernard O. Cholelithiasis in infancy: a study of 40 cases. J Pediatr 1993;122:385–391.
Scholz H, Hofmann T, Noack R, Edwards DJ, Stoeckel K. Prospective comparison of ceftriaxone and cefotaxime forthe short-term treatment of bacterial meningitis in children. Chemotherapy 1998; 44:142–147.
Moyer V, Freese DK, Whitington PF, et al. Guideline for theevaluation of cholestatic jaundice in infants: recommenda-tions of the North American Society for PediatricGastroenterology, Hepatology and Nutrition. J PediatrGastroenterol Nutr 2004; 39:115–128.
Gunnarsdóttir A, Holmqvist P, Arnbjornsson E, KullendorffCM. Laparoscopic aided cholecystostomy as a treatment ofinspissated bile syndrome. J Pediatr Surg 2008; 43:e33–e35.
Political Science 105 Review Legislatures ?? What are the fundamental differences between presidential (separation of powers) and parliamentary (fusion of powers) democracies? ?? Which is more responsive to majorities? Which is more responsive to minorities? Which better reflects the principles of pluralist democracy? Why? ?? What are the basic principles of presidential government
Wenn Sie mich auf dieser Reise begleiten, dann ist, glaube ich, eine Warnung angebracht: Eine manische Depression ist kein friedlicher Sonntagsspaziergang. Sie verläuft nicht nach einem bekannten, vertrauten Muster von A nach B. Sie ist chaotisch und unvorhersehbar. Man weiß nie, wohin sie einen als nächs-tes führt. Ich möchte, dass dieses Buch die Krankheit wider-spiegelt, dass es den Leseri
 284jumonline.qxp:Layout 1 3/17/09 2:30 PM Page 542
Inspissated Bile Syndrome in a Neonate Treated With Cefotaxime
284jumonline.qxp:Layout 1 3/17/09 2:30 PM Page 542
Inspissated Bile Syndrome in a Neonate Treated With Cefotaxime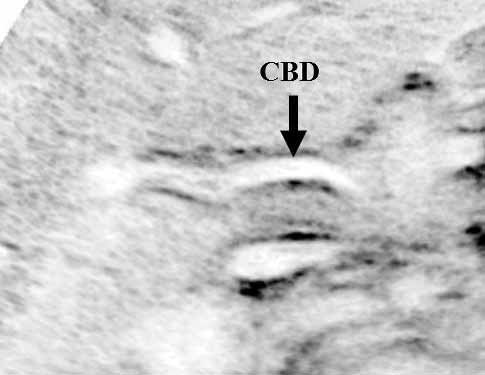 284jumonline.qxp:Layout 1 3/17/09 2:30 PM Page 543
Miloh et al
284jumonline.qxp:Layout 1 3/17/09 2:30 PM Page 543
Miloh et al