Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Casciac.org
Local health departments, school nursing supervisors, school medical advisers, high school wrestling coaches Matthew Cartter, MD, MPH Lynn Sosa, MD Epidemiologist Epidemiologist February 15, 2013 SUBJECT: Information regarding Herpes Gladiatorum infections among high school wrestlers
The Connecticut Department of Public Health (DPH) recently learned of skin infections occurring among high school wrestlers. At least one wrestler has been confirmed to have a herpes infection (known as Herpes Gladiatorum) with several other wrestlers at multiple schools with skin infections that are consistent with this diagnosis. With multiple state and regional tournaments occurring in the next few days and weeks, this communication is meant to alert health care providers, health departments and coaches to these infections so that infections can be promptly identified and treated to prevent further transmission among wrestlers.
Skin infections, including herpes infections, are common among wrestlers. Herpes Gladiatorum is an infection with the virus herpes simplex type-1, the same virus that causes cold sores. Infection is spread by direct skin-to-skin contact and can affect any part of the body with the face and neck most commonly affected among wrestlers. The rash usually occurs within 8 days of exposure (range 2–12 days) and consists of small, often clustered, fluid-filled vesicles surrounded by redness which eventually open up to sores; it is often confused with a bacterial skin infection called impetigo. Some people might experience additional symptoms such as fever, sore throat or swollen lymph nodes. Most infections resolve on their own without any treatment but antiviral treatment can decrease the severity and shorten the length of symptoms. Infections can be more severe if they affect the eye. Herpes infections are lifelong with some people having recurrent rashes that are usually less severe than the initial outbreak but are still infectious to others.
Attached to this letter is a fact sheet on Herpes Gladiatorum as well as guidelines from the National Federation of State High Schools on the treatment, prevention and control of these infections among athletes, including wrestlers. This information should be shared with anyone who assists in the management of high school wrestling teams in the state including student athletes and their parents.
The Epidemiology and Emerging Infections Program at DPH can be contacted at 860-509-7994 with further questions.
Herpes Gladiatorum Fact Sheet 1. What is herpes gladiatorum?
Herpes gladiatorum is a skin infection caused by the herpes simplex virus.
Photos: courtesy of the Minnesota Department of Health
2. How do you get herpes gladiatorum?
This skin infection is spread by direct skin-to-skin contact. Sports that involve close
contact with herpes gladiatorum lesions may spread this infection to other athletes.
3. What is herpes gladiatorum illness like?
Generally, lesions (sores) appear within 8 days after exposure to an infected person, but in some cases it may take longer to appear. Good personal hygiene and
thorough cleansing and disinfecting of all equipment are essential to helping prevent
the spread of this and other skin infections.
All athletes with skin sores or lesions should be referred to a physician or primary care
provider for evaluation and possible treatment. These individuals should not participate in practice or competition until their lesions have healed.
Before skin lesions appear, some people have a sore throat, swollen lymph nodes, fever or tingling on the skin. Herpes gladiatorum lesions appear as a cluster of blisters
and may be on the face, arms, legs or trunk. Seek medical care immediately for
lesions in or around the eye. Every wrestler should be evaluated by a knowledgeable, unbiased adult for the presence of a rash and excluded from practice and
competition if suspicious rashes are present until evaluation and clearance by a
4. What are the serious complications from herpes gladiatorum?
Herpes gladiatorum infections can recur. The virus can “hide out” in the nerves and
reactivate later, causing another infection. Generally, recurrent infections are less
severe and don’t last as long. However, a recurring infection is just as contagious as the original infection, so the same steps need to be taken to prevent infecting others.
5. How can herpes gladiatorum infection be prevented?
Personal hygiene for athletes is essential. • Shower at school immediately after practice, using soap and water.
• Always use your own plastic bottle of liquid soap.
• Wash your towel after each use, using hot water with detergent (and
bleach if possible); and dry on high heat setting.
• Practice and competition gear should be cleaned every day.
• Headgear should be cleaned daily with a bleach wipe or any other
Good hygiene is essential to preventing infection with herpes gladiatorum.
• Hands should be cleaned often! At least 15 seconds washing should be
done using soap and warm water. An alcohol-based hand rub can be used instead of soap if their hands are not visibly soiled.
• Avoid touching your eyes, nose or mouth with your hands.
• Clean your hands before and after practice and competitions. • Never pick or squeeze skin sores; drainage is very infectious.
• Always report any skin lesions or sores to your athletic trainer or coaching
staff immediately, whom in turn should notify teams that they have wrestled in the 8 days prior to an outbreak of herpes gladiatorum and
notify/consult with their school physician immediately so that a treatment
Cleaning and disinfecting the environment is also important in preventing
infection with herpes gladiatorum. Disinfectants approved by the Environmental Protection Agency (EPA) must be used according to
manufacturer recommendations (viricidal, fungicidal, bactericidal) OR bleach
solution (800 ppm = ¼ c bleach: 1 gallon water). Mix daily to be effective. Mats should be washed after every practice session or competition. Locker rooms
and shower areas should be cleaned and disinfected daily using EPA-
approved product or bleach solution. Mop heads and cleaning cloths should be laundered daily using laundry detergent, hot water and dry on high heat
setting. All facilities should be cleaned daily with an appropriate cleaning
agent. This includes locker room, practice room, mats and weight room.
6. How is herpes gladiatorum diagnosed?
Diagnosis is usually based upon appearance and clinical grounds. . If herpes or another
infectious skin lesion is suspected, wrestlers should not practice or play until evaluated by
a competent medical professional. Please contact your primary care provider for specific clinical medical information.
7. For more information on herpes gladiatorum, or skin infections
Additional information (for athletic trainers and clinicians) from the National Federation of State High School Associations (NFSHSA) is available at: Herpes Gladiatorum Position Statement and Guidelines National Federation of State High School Associations (NFHS) Sports Medicine Advisory Committee
In the recent years, control of skin infections has become a crucial part of high school
wrestling. Herpes Gladiatorum (HG), caused by Herpes Simplex Type-1 virus (HSV-1), has received the most attention due to the speed of which it can spread and the long term consequences an athlete may have, even after finishing his/her career. The NFHS Sports Medicine Advisory Committee realizes these issues and has helped establish guidelines to educate the sporting and medical community about their presence, means to treat and reduce transmission of this virus.
Guidelines for Herpes Gladiatorum – Treatment and Prevention
First time Outbreak:
1. Seek medical attention and oral antiviral treatment to expedite its clearance. 2. Regardless if treated, no wrestling until all lesions are healed with well-adhered
scabs. No new vesicle formation and no swollen lymph nodes near area involved.
3. Consider being placed on prophylactic oral antiviral medication for remainder of
Recurrent Outbreaks:
1. Seek medical attention and oral antiviral treatment to expedite its clearance. 2. No wrestling until after 120 hours of oral antiviral medication and no swollen lymph
3. If not treated with antiviral medication, no wrestling until all lesions are healed with
well-adhered scabs. No new vesicle formation and no swollen lymph nodes near area involved.
4. Consider being placed on prophylactic oral antiviral medication for remainder of the season and each subsequent season.
Any individual exposed to the outbreak 3 days prior to its development, should be isolated from direct contact with other athletes for 8 days. Examine them daily for potential Herpes Gladiatorum. Use of antiviral medication for prevention is only at the discretion of your Health Care Provider (HCP), who can then explain the potential risks and benefits.
The spreading of this virus is strictly skin-to-skin with the preponderance of the outbreaks developing on the head, face and neck. This reflects the typical lock-up position a wrestler has facing his/her opponent. Usually a primary outbreak is seen as a raised, rash coalesced into groupings of 6-10 vesicles. Sore throat, fever, swollen, cervical lymph nodes and malaise are typical signs with a first time outbreak. Reoccurrence usually involves a smaller area with less systemic signs and for a shorter duration. Young athletes who contract Herpes Gladiatorum are destined to have a battle with life-long reoccurrences and potential spread to less suspecting individuals, such as partners or children. Differing from recurrent herpes labialis, or ‘cold sores’, recurrent Herpes Gladiatorum can develop around the eye. This location has potential for rare but serious consequences with reoccurrences possibly affecting the visual acuity of the afflicted eye. Previously thought to exist in 2.6% of high school age wrestlers, recent data suggests it may exist in 29.8% of these individuals. Even though this is no different than non-wrestlers in this age group, the location of the outbreaks is of concern. Since only 2-3% of these athletes are aware they have Herpes Gladiatorum, a larger number are competing with the virus and unknowingly exposing it to others. Means of infection control should focus on coaches or Certified Athletic Trainers, performing daily skin checks. An athlete with a suspicious lesion must be withdrawn from practice or competition, only to return after evaluated and cleared by his/her Health Care Provider. Once an outbreak occurs on a team, removing the athlete from competition or play is mandatory to minimize its spread. After being on antiviral medication, and provided no further signs of infection, he/she can return to play. Since the virus can spread before vesicles are present, it’s recommended to examine all athletes in contact with this individual from the previous 3 days. Monitor them for any suspicious lesions, which may take 8 days to develop. Due to the risk of viral spread before vesicle formation, consider isolating these individuals from sparring with others during that time. The usage of oral antiviral medication is beneficial in expediting the clearance of an outbreak. One paper showed that when used for a recurrent outbreak, these medications showed a 2 day reduction in the length of time it takes to clear the virus. Although controversial, the use of prophylactic dosing can help in reducing the reoccurrence of outbreaks. Data exists showing infected individuals to have a greater preponderance to outbreaks when not on the medication. These medications won’t prevent 100% of the outbreaks, but can reduce their occurrence. Amongst health professionals, the concerns about using these medications in this venue center around potential risks, inconsistent benefit and possible resistance development. Documentation exists stating these issues are minimal, yet plausible and need to be mentioned. Therefore, this determination should be done at the discretion of the parents/guardian, Health Care Provider and the athlete. The NFHS Sports Medicine Advisory Committee will continue to promote control of Herpes Gladiatorum by education and raising public awareness about the virus. Affected athletes should work closely with their Health Care Providers to determine the best way to treat an outbreak and how to reduce its spread to other wrestlers. The coaching staff and Certified Athletic Trainers shall focus on: daily skin checks, proper hygienic practices, and withdrawal and treatment of individuals with an active outbreak.
Addendum: Other considerations could be given to perform blood testing to determine antibodies for HSV-1 at the beginning of each season. Anyone who is positive should be considered for daily antiviral prophylaxis throughout the season, even if they have never had a documented outbreak of Herpes Gladiatorum or cold sores. A belief held by few and supported by recent research in high school wrestlers. There is also data to support that shedding of the virus can occur before actual vesicle formation. This would be of importance since present guidelines focus on the presence of vesicles for withdrawal of competition. Prophylaxis would help prevent vesicle formation and possibly reduce viral shedding as these are very important factors in controlling Herpes Gladiatorum transmission. References: Anderson BJ. The Epidemiology and Clinical Analysis of Several Outbreaks of Herpes Gladiatorum. Med. Sci. Sports. Exerc.2003:11:1809-14. Anderson BJ, Clark A, Tillman D. Valacyclovir for Prevention of Reactivation of Herpes Gladiatorum in Wrestlers: an Updated Study. Am J of Med & Sports. Vol. V, No.V, 2003:309-14. Anderson BJ. The Effectiveness of Valacyclovir in Preventing Reactivation of Herpes Gladiatorum in Wrestlers. Clin J Sports Med.1999: Vol. 9, No. 2, 86-90. Anderson BJ. Prophylactic Valacyclovir to Prevent Outbreaks of Primary Herpes Gladiatorum at a 28-day Wrestling Camp. Japanese Journal of Infectious Diseases. 2006:Vol.59, No.1, 6-9.
Anderson BJ. Valacyclovir to Expedite the Clearance of Recurrent Herpes Gladiatorum. Clin J Sports Med. 2005: Vol. 15, No. 5, 364-6.
Becker TM, Kodsi R, Bailey P, et al. Grappling with Herpes: Herpes Gladiatorum. Am. J. Sports Med.1988:16:665-9. Wald A, Zeh J, Selke S, et al. Virology characteristics of subclinical and symptomatic genital herpes infections.1995. N. Engl. J. Med., 333:770-775. Revised and Approved April 2007
Hip International / Vol. 12 no. 4, 2002 / pp. 383-387Early resection of heterotopic ossification after total hip arthroplasty: A review of the literatureDepartment of Orthopedics and Traumatology, Ghent University Hospital, Gent - Belgium ABSTRACT: Early excision of heterotopic ossification was performed in 8 patients at an average of 10.2 months after total hip arthroplasty. All patients re
W . U . S . H E A L T H C E N T R E UNIVERSITY OF DELHI, DELHI-110007 Purchase of Drugs/Medicines & Other items for the year 2011-2012 TENDER NOTICE Sealed tenders are invited from manufactures having G.M.P. certification as per WHO distributors/suppliers having turnover of Rs. Three crore or above per annum (not applicable to Laboratory Chemicals & Glasswares, Dress
 Local health departments, school nursing supervisors, school medical
Local health departments, school nursing supervisors, school medical 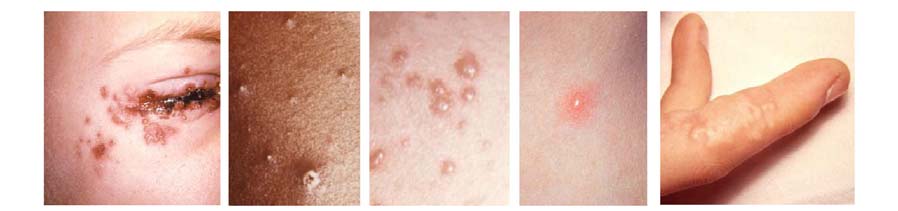 Herpes Gladiatorum Fact Sheet
Herpes Gladiatorum Fact Sheet  Herpes Gladiatorum
Herpes Gladiatorum