Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Microsoft word - swine flu - health alert 4-28-09 _jlj_.doc
State of California—Health and Human Services Agency
MARK B HORTON, MD, MSPH ARNOLD SCHWARZENEGGER SWINE INFLUENZA A (H1N1) HEALTH ALERT Current Situation • As of today, 11 California residents in three counties (San Diego, Imperial and
Sacramento) have been diagnosed with confirmed swine influenza A (H1N1) virus infection; there are also currently four probable cases in these counties under investigation. All but two patients have had self-limited Influenza-like illness (ILI); two patients with underlying conditions were hospitalized. All have recovered.
• Because there was a probable case in a Sacramento school with an epi-link to
another possible case and evidence of other students with ILI, a decision was made to dismiss school until 7 days after the last day an infectious child attended school.
• CDPH has drafted an interim policy on school dismissal and received input from
local Health Officers in a conference call today.
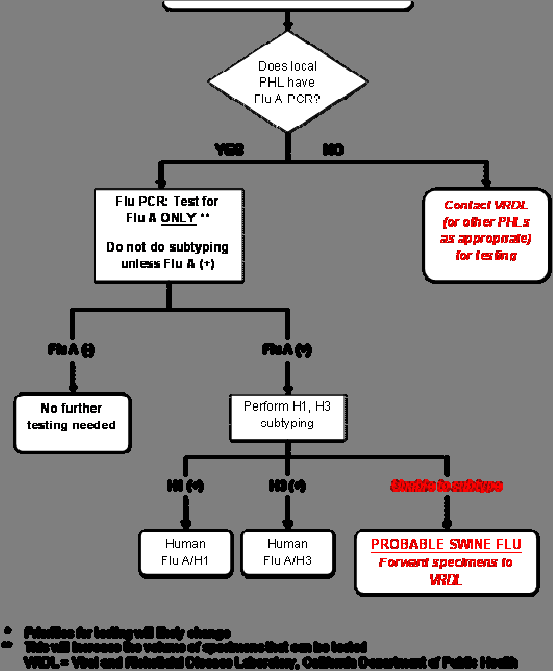
case of swine influenza A (H1N1) virus infection: a person with an
acute respiratory illness with an influenza test that is positive for influenza A, but human H1 and H3 negative (i.e., unsubtypeable).
illness: fever >37.8°C (100°F) and a cough and/or sore throat.
Influenza Surveillance Recommendations Because of the rapidly evolving situation and in an attempt to focus laboratory resources, revised enhanced surveillance guidance is being issued. At this time, testing at public health laboratories should be focused on: • Hospitalized patients with ILI • Outpatients with ILI in the following categories:
o Patient is a contact of a confirmed swine influenza A (H1N1) case o Patient is in a high-risk setting for transmission (e.g., school, prison)
California Department of Public Health, P.O. Box 997377, Sacramento, CA 95899-7377
HEALTH ALERT - California Swine Influenza Page 2 April 28, 2009
o Patient is part of a cluster of people with ILI (only one patient needs
o Patient returned from Mexico within 7 days of illness onset or cared for ill
household members with this travel history
Influenza sentinel surveillance providers should continue submitting specimens according to protocol to the CDPH Viral and Rickettsial Disease Laboratory (VRDL). Any influenza A non-subtypeable results will be reported to the LHD immediately. The CDPH VRDL will continue to support those LHDs that do not have access to PCR testing for influenza as well as local public health laboratories that need assistance with their testing as demand increases. Please alert VRDL if you are sending specimens from patients in any of the above listed categories so testing can be prioritized (e-mail cynthia.jean@cdph.ca.gov and david.cottam@cdph.ca.gov Case and contact investigation Case and contact report forms and laboratory report forms are posted on the CDPH swine influenza website at:http://www.cdph.ca.gov/HealthInfo/discond/Pages/SwineInfluenza.aspx Laboratory Updates: On a statewide call with laboratory directors it was decided that for Northern CA Kaiser patients, specimens from suspect swine influenza cases will first be tested for Flu A at Kaiser Regional Laboratory. Specimens that test positive for Flu A will be forwarded to VRDL for sub-typing. For positive flu A cases, Kaiser will alert the patient’s public health county of residence of positive test result. VRDL has requested a large supply of swabs, viral transport media and shipping boxes. We ask that the local public health laboratories contact us (by e-mailing david.cottam@cdph.ca.go and tong.kong@cdph.ca.gov) with your anticipated supply needs in the next 48 hours. We plan to be sending out those supplies to local public health laboratories within the next few days. All requests from individual hospitals and clinics for specimen collection supplies will be referred to the local health department for assistance. Commercial laboratories do not currently offer swine influenza testing. We are asking that requests for swine influenza testing be triaged at the clinic or hospital laboratory in the following way: HEALTH ALERT - California Swine Influenza Page 3 April 28, 2009 Hospital Prioritization Scheme for Swine Influenza H1 (SwH1) Testing* [rev. 04/27/09] Triage requests for swine influenza testing HIGH-RISK
Patient is a contact of a confirmed swine influenza
(Order Flu A)
Patient is part of a cluster of people with ILI (only one
Patient returned from Mexico within 7 days of illness onset or cared for ill household
* Priorities for testing will likely change
HEALTH ALERT - California Swine Influenza Page 4 April 28, 2009 Specimen collection and algorithm for testing in public health laboratories (See attachments) • Specimen
Please collect one to two respiratory samples (depending on
specimen collection resources) from each patient with ILI. Nasopharyngeal swabs and nasal aspirates are preferable; throat swabs are acceptable if an NP swab or nasal aspirate cannot be obtained. The swabs should be placed in a standard container with 2-3 ml of viral transport media. If the patient is hospitalized with pneumonia, specimens from the lower respiratory tract (e.g., tracheal aspirate, bronchoalveolar lavage) should also be obtained.
• Specimens should be collected within the first 24-72 hours of onset of symptoms
and no later than 5 days after onset of symptoms.
• Specimen storage: The specimens should be kept refrigerated at 4ºC and sent on
cold packs if they can be received by a public health laboratory within five days of the collection date. If samples will be received by the laboratory in five or more days from collection, they should be frozen at -70 ºC or below and shipped on dry ice.
o Viral transport media o Mask and gloves
*Cotton or calcium alginate swabs are not acceptable. PCR assays may be inhibited by residues present in these materials
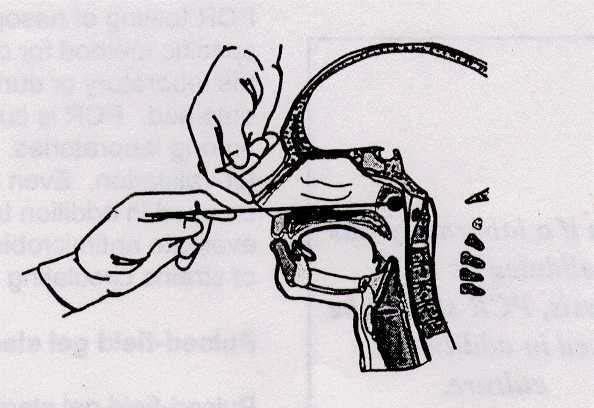
Procedure: 1. Put on mask and gloves. 2. Have patient sit with head against a wall as patients have a tendency to pull
3. Insert swab into one nostril straight back (not upwards) and continue along the
floor of the nasal passage for several centimeters until reaching the nasopharynx (resistance will be met). The distance from the nose to the ear gives an estimate of the distance the swab should be inserted. Do not force swab, if obstruction is encountered before reaching the nasopharynx, remove swab and try the other side.
4. Rotate the swab gently for 5-10 seconds to loosen the epithelial cells. 5. Remove swab and immediately inoculate viral transport media by inserting the
swab at least ½ inch below the surface of the media. Bend or clip the wire swab handle to fit the transport medium tube and reattach the cap securely. A dry swab is not acceptable for PCR testing.
HEALTH ALERT - California Swine Influenza Page 5 April 28, 2009
6. Specimen should be transported at refrigerator temperature and received by
laboratory as soon as possible and <3 days from time of collection.
For a video of NP swab collection, please see: http://video.cdc.gov/asxgen/nip/isd/swabdemo.wmv
Infection Control Precautions CDPH concurs with CDC’s “Interim Guidance for Infection Control for Care of Patients with Confirmed or Suspected Swine Influenza A (H1N1) Virus Infection in a Healthcare Setting,” April 24, 2009, which can be accessed at: http://www.cdc.gov/swineflu/guidelines_infection_control.htm Recommendations for antiviral therapy and prophylaxis for swine influenza A (H1N1) These recommendations are subject to change based on current conditions CDPH concurs with the Center for Disease Control and Prevention’s (CDC’s) current “Interim Guidance on Antiviral Recommendations for Patients with Confirmed or Suspected Swine Influenza A (H1N1) Virus Infection and Close Contacts,” which can be accessed at: http://www.cdc.gov/swineflu/recommendations.htm This guidance refers to the current recommended daily dosage of influenza antiviral medications for treatment and chemoprophylaxis. Higher doses of oseltamivir (e.g., 150 milligrams twice daily) may be considered on a case-by-case basis in severe swine influenza A (H1N1) infections, particularly if there is pneumonic disease at presentation or evidence of clinical progression. There is HEALTH ALERT - California Swine Influenza Page 6 April 28, 2009 currently no evidence for enhanced efficacy of high-dose oseltamivir therapy in swine A (H1N1) infections, but this recommendation aligns with World Health Organization Advice for Avian Influenza A (H5N1) infections. High-dose therapy appears to offer no additional benefit for the treatment of seasonal influenza. Other CDC Guidance Documents
Interim Guidance for Swine influenza A (H1N1): Taking Care of a Sick Person in Your Home, April 25, 2009. http://www.cdc.gov/swineflu/guidance_homecare.htm Interim Recommendations for Facemask and Respirator Use in Certain Community Settings Where Swine Influenza A (H1N1) Virus Transmission Has Been Detected, April 26, 2009. http://www.cdc.gov/swineflu/masks.htm Swine Influenza A (H1N1) Virus Biosafety Guidelines for Laboratory Workers, April 24, 2009. http://www.cdc.gov/swineflu/guidelines_labworkers.htm Community Strategy for Pandemic Influenza Mitigation February 2007 http://www.pandemicflu.gov/plan/community/commitigation.html
HEALTH ALERT - California Swine Influenza Page 7 April 28, 2009
Investigación original / Original research Initiation of effective postpartum contraceptive use in public hospitals in Guatemala Edgar Kestler,1 Maria del Rosario Orozco,2 Silvia Palma,2and Roberto Flores 2 Suggested citation Kestler E, Orozco MR, Palma S, Flores R. Initiation of effective postpartum contraceptive use in publichospitals in Guatemala. Rev Panam Salud Publica. 2011;29(2):
Physicians Plus Insurance Corporation Drug Formulary Website: www.pplusic.com Last Updated 7/08 This is a summary by category of formulary alternatives. Physicians Plus reserves the right to change the formulary at any time. When an acceptable generic is available, the generic productis considered the covered, formulary product. Prior Authorization FAX # 608-258-1905, Pharmacy Services phone #



 State of California—Health and Human Services Agency
MARK B HORTON, MD, MSPH
State of California—Health and Human Services Agency
MARK B HORTON, MD, MSPH