Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Ftp.ccss.sa.cr
C H A P T E R 3 Coccidian Parasites Cyclospora cayetanensis, Isospora belli,3.1 PREFACE Cyclospora cayetanensis, Isospora belli, and the Sarcocystis spp. Sarcocystis homi-nis and Sarcocystis suihominis are parasites that infect the enteric tract of humans(Beck et al., 1955; Frenkel et al., 1979; Ortega et al., 1993). These parasites causedisease when infectious oocysts are ingested by humans. The routes of transmissioncan be direct human to human contact or through contaminated food (Connor andShlim, 1995; Fayer et al., 1979) or water (Wright and Collins, 1997). Taxonomically,these parasites are very distinct: Cyclospora and Isospora belong to the Eimeriidaes,whereas Sarcocystis belongs to the Sarcocystidae. Nonetheless, some similaritiesare noteworthy: infectious stages of these parasites have morphological similarities,they have been reported to be food-borne, they cause infections of the intestinaltract of humans, and their clinical presentations have similarities (Mansfield andGajadhar, 2004). Thus, relatedness and differences between several aspects of cy-closporiasis, isosporosis, and sarcocystosis will be covered in this chapter. 3.2 BACKGROUND/HISTORY Cyclospora is probably the most important foodborne pathogen of the three parasites. It is endemic in several regions of the world, primarily in developing countries(Markus and Frean, 1993; Ortega et al., 1993), whereas in the developed world ithas been associated with important foodborne outbreaks (Charatan, 1996; Herwaldt,2000; Herwaldt and Beach, 1999). It has also been reported in travelers returningfrom endemic areas (Gascon et al., 1995; Soave et al., 1998). Isospora belli is an infrequent parasite of humans, with most cases reported from
tropical areas. In the immunocompetent population, Isospora infections are usuallyasymptomatic (Teschareon et al., 1983). Immunocompromised patients, however,can suffer I. belli infections associated with severe clinical disease (Soave, 1988).
Human sarcocystiosis is even more infrequent, and infectious parasites are in-
cidentally identified in feces (Bunyaratvej et al., 1982; Fayer, 2004). The clinicalsignificance of the detection of oocysts or sporocysts in feces is unknown in mostcases (Dubey, 1993) . Cyclospora cayetanensis was fully recognized as a parasite less than 15 years ago
(Ortega et al., 1993), and gained significant recognition because of its associationwith several food-borne outbreaks in the United States. The name and description
of human infectious Cyclospora dates back to 1992, however, previous studiesdescribed organisms similar to Cyclospora. One of the oldest, if not the first doc-umented report was published in 1979 (Ashford, 1979), describing a parasite withmicroscopic characteristics of immature (nonsporulated) C. cayetanensis oocysts. This report concluded that the described organism probably was a new species ofIsospora infecting humans (Ashford, 1979).
In the following years, other investigators reported the organisms autofluoresced
when observed under UV light (Long et al., 1991). This finding led some inves-tigators to believe it was a blue-green algae or a cyanobacterium. Thus, the termcyanobacterium-like body or CLB was coined and used for some years. Other termsfound in the literature that also referred to Cyclospora were coccidian-like body(also CLBs) (Hoge et al., 1993) or big Cryptosporidium, as reported by Naranjoet al. in the 1989 Annual Meeting of the American Society of Tropical Medicineand Hygiene. Findings in this report were on the basis of microscopy of acid-faststained organisms and transmission electron micrographs that showed sections oforganisms resembling encysted flagellates.
Shortly thereafter, studies led by Ortega demonstrated that CLBs were indeed
a coccidian parasite, with each oocyst containing two sporocysts, and each of themcontaining two sporozoites. These findings were first presented at the Annual Meet-ing of the American Society of Tropical Medicine and Hygiene in November 1992. The morphological characteristics of the parasite allowed its classification as a pro-tozoan parasite belonging to the genus Cyclospora (Ortega et al., 1993). Shortlythereafter, the parasite was named C. cayetanensis, in honor of Universidad PeruanaCayetano Heredia, a Peruvian University where preliminary studies were conducted(Ortega et al., 1994). Thus far, it is the most recently recognized coccidian parasiteaffecting humans.
In contrast to Cyclospora, Sarcocystis, and Isospora have been known to in-
fect humans for several decades. I. belli is an enteric parasite exclusively fromhumans (Ferreira et al., 1962; Panosian, 1988). Although it infects, replicates, andcompletes its life cycle in enteric epithelial cells, it does not cause any signifi-cant disease in the immune-competent population. People with impaired immu-nity, however, may develop extra-intestinal infections and isosporiasis may posea risk to their lives (Arnaud-Battandier, 1985; Figueroa et al., 1985; Furio andWordell, 1985; Henry et al., 1986; Jonas et al., 1984; Kobayashi et al., 1985; Maet al., 1983; Modigliani et al., 1985; Ng et al., 1984; Ros et al., 1987; Shein andGelb, 1984; Whiteside et al., 1984) (Table 3.1). Sarcocystis spp. were first reported by Miescher in 1843, who described white
milky lesions in the muscles of house mice. Since the initial report, multiple authorsdescribed similar lesions and infections in the flesh of various animal species. Thetransmission cycle, however was not yet elucidated. In 1943, Scott demonstratedthat there was no direct transmission from infected to healthy sheep. Despite thenegative results, it gave an indication that there was no direct transmission betweenmembers of the same species. It took several decades until the life cycle of S. hominisand S. suihominis were finally described in the 1970s (Heydorn, 1977; Rommel andHeydorn, 1972), when it was demonstrated that both of these parasites required two
Table 3.1. Similarities and differences between Cyclospora, Sarcocystis, and Isospora species that infect humans. Life cycle Epidemiology
Opportunisticinfection in immuneimpaired people
Symptoms
Stage found in stools Unsporulated oocysts
hosts: a definitive host; also described by others as the predator species, and anintermediate host or prey. Infections in the definitive hosts usually infect the enterictract, where asexual and sexual stages develop. In contrast, in intermediate hosts theparasites develop sexual stages only, forming white milky threads (sarco = flesh andkystis = bladder) in their muscles. Shortly thereafter in 1975, it was demonstratedthat cattle and sheep could be the intermediate hosts for more than two species ofSarcocystis, and that simultaneous infections may occur (Heydorn et al., 1975). 3.3 BIOLOGY
The oocysts of C. cayetanensis are spherical, with 8–10 μm in diameter, and althoughits life cycle has not been fully demonstrated, evidence so far supports the notion thatthis is a parasite that only infects humans (Ashford, 1979; Ortega et al., 1994; Ortegaet al., 1993). Cyclospora has been reported in feces of some animal species, includingducks (Zerpa et al., 1995), chickens (Garcia-Lopez et al., 1996), dogs (Carollo et al.,2001; Yai et al., 1997), and monkeys (Chu et al., 2004); however, no evidence of tis-sue infections was described in these animals. Cyclospora spp. were observed in non-human primates and genetic analysis based on the small subunit RNA gene revealedsignificant host specificity. Cyclospora papionis was exclusively found in baboons,vervet monkeys were only infected with Cyclospora cercopitheci, and only colobusmonkeys had infections with Cyclospora collobi (Eberhard et al., 2001). Animalinfectivity studies using nine strains of mice, including adult and neonatal immuno-competent and immune-deficient inbred and outbred strains, rats, sandrats, chickens,ducks, rabbits, jirds, hamsters, ferrets, pigs, dogs, owl monkeys, rhesus monkeys,and cynomolgus monkeys, were unsuccessful. These findings suggest that C. cayeta-nensis is a species specific parasite that only infects humans (Eberhard et al., 2000).
There are two species of Sarcocystis that can infect humans, S. hominis and
S. suihominis. As their names suggest, these are two-host parasites and man becomes
infected by ingesting viable cysts in the meat of bovids or swine, respectively. Oocysts of these parasites are indistinguishable by microscopy; elliptical in shape,measuring 13 by 10 μm. Two sporocysts develop and in contrast to Cyclospora, theoocyst wall is fragile and usually ruptures, so that the sporocysts are more commonlyfound in clinical specimens and in the environment. Isospora oocysts are elliptical, measuring 20–30 μm by 10–20 μm. These
oocysts are shed unsporulated into the environment; thus, clinical specimens frompatients will contain eplitical red structures when stained with acid fast. In environ-mental samples, however, the sporulated forms are likely to be found. Within theoocysts wall, two spherical structures can be observed. Initially they are called spher-oblasts, and when mature, sporocysts. Each sporocyst will be spherical in shape,measuring 10–12 μm in diameter and will contain four sporozoites each. Cyclospora and Isospora are believed to be monoxenus parasites, infecting only
humans. Infectious stages of Cyclospora have been identified in the small intestine,although the complete life cycle has only been postulated. Sarcocystis are commonly found in several species of farm animals. Of public
health importance are S. hominis and S. suihominis. People acquire these parasitesby ingesting raw or undercooked infected beef or pork.
The life cycle of these parasites is very different. While Cyclospora and Isospora
are reported to be anthroponotic, meaning these parasites complete their life cyclesexclusively in humans, Sarcocystis parasites have a more complex life cycle andrequire two different hosts: an intermediate bovid in the case of S. hominis, and pigsfor S. suihominis. In both cases, humans are the definitive host.
Human infections of these parasites affect the digestive tract. Cyclosporiasis
starts after a susceptible host ingests sporulated oocysts, the infectious stage. After
ingestion, oocysts are ruptured in the upper gastrointestinal tract and the two sporo-cysts are liberated. Shortly thereafter, two sporozoites are released from each sporo-cyst and proceed to infect epithelial cells of the intestine. The extent of infectionin the human gastrointestinal tract has not been clearly determined. Ortega and col-laborators (Ortega et al., 1997a) have described intracellular stages from histologi-cal sections of upper gastrointestinal biopsies from 17 Peruvian patients. Meronts,macrogametocytes, and microgametocytes were identified in the cytoplasm of jeju-nal enterocytes, demonstrating that oocysts could be formed in this section of theenteric lumen. The extent of intestinal infection or preferential site of infection hasyet to be reported. This apparent lack of information is in part due to the absence of ananimal model to study human cyclosporiasis (Sadaka and Zoheir, 2001). Laboratorystudies have attempted to infect immunocompetent and immunodeficient animalswhich were unsuccessful, and none of these species developed clinical symptomsor patent infections (Eberhard et al., 2000).
There are anecdotic reports of Cyclospora in ducks (Zerpa et al., 1995), dogs (Yai
et al., 1997), chickens, and monkeys found naturally infected with Cyclospora (Chuet al., 2004). Observed using acid fast stain, coccidian-like bodies were described inthe stools of a duck owned by a Cyclospora-infected patient, while fecal droppingsfrom ducks of noninfected people were Cyclospora negative (Zerpa et al., 1995). Although two dogs in Sao Paulo, Brazil were reported positive for Cyclospora, afollow-up study of 140 dogs from the same city did not find any infected dogs(Carollo et al., 2001). Recently, dogs, chickens, and monkeys from Nepal werefound microscopy positive for Cyclospora and these samples were further con-firmed by polymerase chain reaction (PCR). The authors concluded that infectionsin these species needed further confirmation including histological demonstrationof infectious stages (Chu et al., 2004).
Seventeen Peruvian patients positive for Cyclospora organisms were surveyed
and underwent endoscopy, and their symptoms were recorded. Patients presentedwith gastrointestinal symptoms, including diarrhea, flatulence, weight loss, abdomi-nal discomfort, and nausea. Jejunal biopsies showed an altered mucosal architecturewith shortening and widening of the intestinal villi due to diffuse edema and infil-tration by a mixed inflammatory cell infiltrate. There was reactive hyperemia withvascular dilatation and congestion of villous capillaries. Parasitophorous vacuolescontained sexual and asexual forms. Type I and II meronts, with 8–12 and 4 fullydifferentiated merozoites, respectively, were found at the luminal end of epithelialcells. These findings demonstrated the complete developmental cycle associatedwith host changes due to C. cayetanensis (Ortega et al., 1997a).
Microscopy studies of human tissues infected with sarcocysts revealed the com-
plexity of this parasite. Lesions from 40 patients were studied by histopathology,revealing seven morphological types of the parasite. Each type represented one toseveral different species, all of which were zoonotic. Among four types of sarcocystsfound in skeletal muscle, three closely resembled a corresponding species foundcommonly in monkeys: one from a man in Uganda, another from an Indian patient,and one from a patient in Southeast Asia. Among three types of sarcocysts found inthe human heart, one resembled a species commonly seen in the heart of cattle. Of
the 40 Sarcocystis infections in man, 13 probably were acquired in Southeast Asia,8 in India, 5 in Central or South America, 4 each in Africa and Europe, 3 in US, 1 inChina and 2 from unknown localities. Symptoms associated with these infectionsincluded muscle soreness or weakness, subcutaneous swellings, eosinophilia, andperiarteritis or polyarteritis nodosa. Nonetheless, there is no conclusive evidence ofpathogenicity of the mature sarcocyst (Beaver et al., 1979).
Occasionally, local infections may present complications due to large localized
inflammatory reactions. Eight out of 11 presented with infections of the tongue andnasopharynx (Pathmanathan and Kan, 1992). Potential association with vasculitishas also been proposed (McLeod et al., 1980).
Infections with I. belli are found worldwide, but are more frequent in tropical and
subtropical areas. Immunocompetent people usually have asymptomatic disease,while immunocompromised persons develop chronic diarrhea and extraintestinalinfections. The life cycle of this organism stars with the excertion of unsporulatedor partially sporulated occysts. Upon sporulation, which can occur as fast as 24hours, the oocysts become infectious. The cycle continues when a person ingestsinfectious oocysts and the sporozoites are released in the small intestine. There,Isospora infects enterocytes, undergoes asexual and sexual reproduction. Leadingto the production and shedding of I. belli unsporualted or partially sporulated oocysts,also known as sporoblasts (Lindsay et al., 1997). 3.4 CLINICAL SIGNIFICANCE
Diarrhea, malaise, lack of energy, and appetite are symptoms associated with severalgastrointestinal pathogens, and are present in patients with cyclosporiasis in devel-oped countries. In endemic areas, clinical infections are usually detected in children4–10 years of age. About 50% of these children present with diarrhea and othergastrointestinal discomforts, including malaise, bloating, and anorexia. Infectionsmay resolve spontaneously, suggesting that immunity may play a role in clearanceof infections.
In the case of human isosporiasis, severe symptoms have been reported in AIDS
patients or people with other forms of immune-suppression. The most frequentlyclinical symptoms are fever, malaise, chronic and persistent diarrhea, steatorrhea,and loss of weight. The infection can even cause death.
Clinical disease associated with human sarcocystosis is usually limited
(Dissanaike, 1994; Pozio, 1991), and most human infection studies demonstratedspontaneous resolution within a month postinfection (Chen et al., 1999). Infectionstudies in humans (Lian et al., 1990) reported clinical symptoms such as anemia, ab-dominal pain, diarrhea, fatigue, and dizziness on day 3 postinfection. Sporocysts andoocysts were found in the feces on day 8. The patent period of sporocyst excretionwas more than 42 days. In addition to digestive malaise, another symptom associ-ated with Sarococystis infections may be muscle aches (Pamphlett and O’Donoghue,1990).
Experimental infections using human volunteers have been reported in the litera-
ture. Eight medical students ate raw meat from a pig experimentally infected with S.suihominis. Six to twenty-four hours after the meal all persons suffered from acuteclinical symptoms, particularly diarrhea and vomiting, and coldness and sweatingwhich decreased by the second day (Piekarski et al., 1978). At the Institute of Med-ical Parasitology, University of Bonn, eleven medical students and six members ofthe institute participated in a meal with raw pork of an experimentally S. suihominisinfected pig. Only individuals who ingested excessively high quantities of infectedmeat suffered severe symptoms (Kimmig et al., 1979).
No serological associations were found between heart conditions and Sarco-cystis infections in Egypt (Azab and el-Shennawy, 1992), but serological evidenceassociates this disease with chronic fatigue syndrome (Pamphlett and O’Donoghue,1992).
Twenty-two intestinal specimens surgically resected due to segmental entero-
colitis were classified into three groups: (1) acute inflammation with hemorrhageand necrosis; (2) constrictive lesion; and (3) false diverticulum with perforation. Thepredominant finding was unisegmental involvement, distributed in jejunum, ileum,and ileocolon. Microscopically, small parasitic structures, interpreted to be an un-conventional excystation stage of S. hominis, were present on the luminal borderand within the crypt-lining epithelial cells (Dubey, 1976). At the ulcerated area,tissue invasion by Gram-positive bacteria were consistently seen and considered assecond pathogen (Bunyaratvej and Unpunyo, 1992). 3.5 TRANSMISSION AND EPIDEMIOLOGY 3.5.1 Cyclospora Foodborne outbreaks in the United States have increased in absolute numbers over the past 30 years. Data analysis from the Foodborne Outbreak Surveillance System revealed 190 outbreaks between 1973 and 1997. During this period, Cyclospora and E. coli O157:H7 were newly recognized causes of foodborne illness (Sivapalasingam et al., 2004). Cyclospora cayetanensis infections, thus far, have only been confirmed in hu-
mans. Currently, no animal species is considered to be an intermediate or accidentalhost, or a reservoir of C. cayetanensis. Epidemiological studies have demonstratedtransmission through the foodborne route. Surveys of fresh produce were conductedin an endemic area, detecting Cyclospora in 1.8% of the samples (Ortega et al.,1997b).
Results from studies to determine waterborne transmission of Cyclospora are
controversial. The first report came from Nepal, where contaminated chlorinatedwater was identified as the source of Cyclospora infections between expatriates inNepal (Rabold et al., 1994). A retrospective epidemiological investigation of anoutbreak within a hospital in IL identified drinking water as the source of infection(Huang et al., 1995). A prospective epidemiological study in Haiti (Lopez et al.,2003) reported variations in the percentage of cases of Cyclospora infections, from12 to 1.1 % between February and April 2001. One artesian well was positive priorto this study; however, none of the wells was positive thereafter. Therefore, no epi-demiological associations were established between infections and water sources.
Molecular investigations have reported the detection of parasite DNA in surfacewater from California (Dowd et al., 2003; Shields and Olson, 2003). These find-ings indicate that Cyclospora may indeed be present in water and that water bornetransmission needs to be further studied.
Currently, Cyclospora is primarily considered a food-borne parasite, although
before 1996, cyclosporiasis was originally considered a diarrheal disease affectingreturning travelers.
This concept changed in the spring of 1996, when a large food-borne outbreak
of cyclosporiasis occurred in North America, affecting 1465 people from 20 states,the District of Columbia, and two provinces (Herwaldt and Ackers, 1997). Epidemi-ological investigations confirmed the vast majority of cases were associated with55 events that served raspberries. This investigations later demonstrated a signifi-cant association between cyclosporiasis and consumption of raspberries importedfrom Guatemala (Herwaldt and Ackers, 1997). Detailed epidemiological descrip-tions of specific events included a wedding reception in Massachusetts (Fleminget al., 1998), and a luncheon in Charleston, S.C. where 38 of 64 attendees met thecase definition of cyclosporiasis (Caceres et al., 1998). Cluster investigations inFlorida showed that raspberries were the only food common to this outbreak andconfirmed them to be imported from Guatemala as well (Katz et al., 1999).
In the spring of 1997, another large outbreak of cyclosporiasis affected the USA
and Canada. Epidemiological and trace-back investigations identified 41 infectionclusters that comprised 762 cases of acute cyclosporiasis and 250 sporadic casesof cyclosporiasis. Similar to the 1996 outbreak, there were significant associationsbetween Cyclospora infections and consumption of Guatemalan raspberries. As aconsequence of this second outbreak, exportation of Guatemalan raspberries wasvoluntarily suspended in May 1997 (Herwaldt and Beach, 1999).
Other fresh produce has been implicated in the transmission of Cyclospora.
Basil was directly implicated in a 1999 outbreak in Missouri, where 62 cases wereidentified. All of these people had previously eaten either pasta chicken salad at oneevent or tomato basil salad at another event (Lopez et al., 2001). European coun-tries also have documented cases of foodborne cyclosporiasis. Although a specificvegetable was not identified, the foods associated with disease risk was lettuce im-ported from southern Europe that was spiced with fresh green herbs (Doller et al.,2002).
Recently, snow peas have been implicated as sources of transmission of cy-
closporiasis. A recent outbreak found that 50 potential cases of cyclosporiasis werelinked to the consumption of snow peas imported from Guatemala (Anonymous,2004). Cyclospora infections had been previously reported in travelers returning from
developing countries. Although infections have been reported from Southeast Asia,Papua New Guinea, Indonesia, India, Pakistan, Nepal, the Middle East, North Africa,the United Kingdom, the Caribbean, the United States, Central America, and SouthAmerica, the true prevalence of this parasite in any population is unknown. Infectionswere reported in travelers returning from South America (Drenaggi et al., 1998). In1997, Cyclospora was reported in 5 of 469 returning travelers with diarrhea (Jelineket al., 1997). Among expatriots living in endemic areas, a study in Nepal reported a
higher risk of diarrhea among foreigners during the first 2 years of residence (Shlimet al., 1999).
Endemic cyclosporiasis has been reported in several areas of the world, mainly
in developing countries. Although there are socioeconomical and geographical sim-ilarities with other related pathogens including Cryptosporidium, Giardia, and bac-terial and viral disease, there are also marked differences. In general, Cyclospora hasbeen reported affecting children in areas where access to clean water or sanitationis marginal or suboptimal. A prospective study in Peru found that children betweenthree and six years of age were more frequently affected (Bern et al., 2002), andinfections were rare after 10 years of age. These findings suggest that humans livingin endemic areas where exposure to the parasite is frequent can develop protectiveimmunity.
These observations, however, are limited to specific areas where the parasite is
endemic. Another study on upper-middle-class Peruvians, showed that this popula-tion presents sporadic disease which closely resembles cyclosporiasis in developedcountries (Ortega et al., 1997a). Although the study sites were only a few milesapart, the sanitary infrastructure was markedly different, emphasizing the role ofsanitation as an important factor for cyclosporiasis.
Endemic cyclosporiasis has been reported around the world. The first report sug-
gested that Cyclospora infections were more commonly found in children, (Ortegaet al., 1993) especially those under 5 years of age (Hoge et al., 1995). In LatinAmerica, Cyclospora infections have been reported in children with diarrhea inBrazil (2/315) (Ribes et al., 2004) and 6.1% of people living in impoverished areasin Venezuela (Chacin-Bonilla et al., 2003). A study conducted with 36 case and 37control Egyptian children reported Cyclospora infections in 5.6% of malnourishedchildren compared to 2.8% of the controls (Rizk and Soliman, 2001). Cyclosporais not considered an HIV opportunistic agent, with similar incidence rates amongimmunocompromised and immunocompetent people. Nonetheless, a recent studyin Egypt reported 6% Cyclospora among Hodgkins Lymphoma patients receivingchemotherapy (Rizk and Soliman, 2001). Additionally, Cyclospora infections werereported in 7 of 71 Venezuelan HIV infected patients and 7 of 132 otherwise normalchildren ages 1–12, while the highest frequency was observed in children 2–5 yearsof age (Chacin-Bonilla et al., 2001).
An epidemiologic study among Guatemalan children reported significant differ-
ences in the epidemiology of Cyclospora in Guatemala. Cyclospora was detected in117 (2.1%) of 5520 specimens, mainly in children 5 years of age. Cyclospora infec-tions were more strongly associated with diarrhea than Cryptosporidium infections(Bern et al., 2000). Cyclospora was also reported in 1.5% of Guatemalan people,however, none of the infected cases were raspberry farm workers (Pratdesaba et al.,2001).
Findings from a three-year longitudinal study (1995–1998) in children living in
an impoverished area of Peru, showed an incidence rate of 0.20 cases per child-year,which was constant among children 1–9 years of age. Infections were more frequentduring the warmer months, December to May, showing a seasonal pattern (Bernet al., 2002). C. cayetanensis oocysts were also detected in 1.1% of 5836 Peruvianchildren studied over 2 years (Madico et al., 1997). A longitudinal study in several
areas of Nepal from April 1995 to November 2000 found marked seasonality, withhighest infection rates occurring during the summer and rainy season of the year(Sherchand and Cross, 2001).
Additional studies have reported endemic cyclosporiasis on all continents, pri-
marily affecting children. A study in Lagos, Nigeria, reported an overall prevalenceof 0.9% (Alakpa et al., 2002, 2003). In Yunnan, China, 5.29% of pediatric diar-rhea cases had Cyclospora (Zhang et al., 2002). In 2002, Uga found Cyclospora inthe Bekasi District in West Java, Indonesia (Uga et al., 2002). Cyclospora infec-tions have been reported in pediatric and adult patients with diarrhea in Tanzania(Cegielski et al., 1999) and the sub-Saharan region (Markus and Frean, 1993). 3.5.2 Isospora Isospora belli infections are infrequently reported in humans, however, patients with impaired immune systems may develop chronic life-threatening diarrhea. Within this population, there has been a sharp drop in the incidence of isosporiasis due to the prophylactic use of trimethropin sulfamethoxazole. The clinical, transmission, and epidemiological features of human isosporiasis are usually found in the form of case reports.
Human isosporiasis affecting immunocompetent people is very rare. In the
United States, a review of human stools received in Kentucky clinics from Marchto September 2003 did not detect Isospora positive specimens (Ribes et al., 2004). Similar findings were reported from Japan, where a 7-year study of 4273 specimenscollected from patients with infectious enteritis and admitted to hospitals found onlythree positive samples (Obana et al., 2002). In developing countries, however, I . belli has been reported in children with diarrhea (Tavarez et al., 1991).
In patients with AIDS-associated complications, I. belli infections accompanied
by chronic diarrhea and wasting were reported in people not receiving or withsubtherapeutic plasma levels of antiretroviral medications (Brantley et al., 2003;Maiga et al., 2002). In developing countries, the prevalence of I. belli infections inHIV-infected patients varies from 1.5 to 17% (Brandonisio et al., 1999; Cimermanet al., 1999; Cranendonk et al., 2003; Ferreira, 2000; Gassama et al., 2001; Joshiet al., 2002; Lainson and da Silva, 1999; Lebbad et al., 2001; Mohandas et al., 2002;Wiwanitkit, 2001).
Severe Isospora infections have also been reported in patients with neoplastic
diseases (Makni et al., 2000; Resiere et al., 2003) and chronic renal failure (Aliet al., 2000). 3.5.3 Sarcocystis Despite its biological similarities with Toxoplasma and Isospora, Sarcocystis is not considered an AIDS-opportunistic infection (Dionisio et al., 1992). Most reports of cases of Sarcocystis in animals and humans are from Asia.
Reports of human infections with Sarcocystis are limited. Most of them are fromAsia. In Thailand, six patients aged 3 to 70 years presented with acute enteritisassociated with Sarcocystis infection (Bunyaratvej et al., 1982).
In Tibet, fecal specimens of 926 persons from Duilongdeqing, Milin, and Linzhi
counties were examined. The prevalences of S. hominis in the three counties were20.5, 22.5, and 22.9% respectively, with an average of 21.8%. S. suihominis preva-lence was 0, 0.6, and 7.0% respectively. No significant difference in infection ratewas found between different age or sex groups. Sarcocystis was detected in 42.9%of beef specimens from markets. The infected cases were generally asymptomatic(Yu, 1991).
In Malaysia, Sarcocystis cysts have been reported from domestic and wild an-
imals, including domestic and field rats, moonrats, bandicoots, slow loris, buffalo,and monkey. The overall seroprevalence in humans was 19.8% among the mainracial groups in Malaysia (Kan and Pathmanathan, 1991). Sarcocystis sp. was identified in 14 Vietnamese individuals from a total of 1228
examined (1.1%) who came to Central Slovakia in the course of 18 months in1987–1989. The subjects were from the north eastern part of the country fromHanoi-Haiphong areas (Straka et al., 1991).
Three cases of muscular sarcocystosis from West Malaysia were reported. Eight
of 11 cases were associated with malignancies, especially of the tongue and na-sopharynx (Pathmanathan and Kan, 1992).
The prevalence of human skeletal muscle sarcocystosis in Malaysia was deter-
mined by examination of tongue tissues from autopsies of subjects aged 12 yearsor more. Of 100 tongues examined, 21% were found to contain Sarcocystis. Thenumber of cysts per case varied from 1 to 13. The age range of positive cases wasfrom 16 to 57 years (mean 37.7 years). Prevalence did not differ with regard to race,sex, or occupation (Wong and Pathmanathan, 1992). Sarcocystis sp. was identified in 23.2% of 362 Thai laborers who were going
abroad for work. Sarcocystis were frequently found in male laborers (83.3%) ( p <0.01). The laborers from northeastern Thailand (n = 278) had a higher prevalence(26.6%) of Sarcocystis infection ( p < 0.01) (Wilairatana et al., 1996).
Fifty samples of raw kibbe from 25 Arabian restaurants in the city of Sao Paulo,
Brazil, were examined for the presence of Sarcocystis. Sarcocysts was found in all50 samples. Based on cyst wall structure, S. hominis (94%), S. hirsuta (70%), andS. cruzi (92%) were identified; mostly as mixed infections (Pena et al., 2001).
A patient from West Malaysia presented with Sarcocystis in the larynx (Kutty
and Dissanaike, 1975). Sarcocystis was identified in biopsy specimens from twoadults in Singapore, one in Bombay, one in Uganda, and in the heart of a child inCosta Rica. Among the sarcocysts seen in the 40 cases (35 old and 5 new), sevenmorphological types were recognized, each representing one to several differentspecies, all of which are zoonotic. Of the 40 Sarcocystis infections in man, 13probably were acquired from Southeast Asia, 8 from India, 5 from Central or SouthAmerica, 4 each from Africa and Europe, 3 from USA, 1 from China, and 2 fromunknown localities (Beaver et al., 1979; Gut, 1982).
In Czechoslovakia, Sarcocystis cruzi, Sarcocystis hirsuta and S. hominis were de-tected in 87% of 200 cattle and Sarcocystis ovicanis and Sarcocystis tenella in 92%of 100 sheep examined. All of 200 pigs examined were negative (Gut, 1982).
In New Zealand, muscle tissue from the oesophagus and diaphragm of 500 beef
cattle were examined. All cattle were infected with Sarcocystis: 98% had S. cruziand 79.8% had S. hirsuta/S. hominis (Bottner et al., 1987).
In Belgium, muscle tissue from the oesophagus, diaphragm, and heart of 100
cattle were examined for Sarcocystis infection. Of these, 97% were positive. Thick-walled cysts were recovered from 56% of animals, but these could not be identifiedas S. hirsuta and/or S. hominis on morphological grounds (Vercruysse et al.,1989).
In India, muscle samples from 890 slaughtered pigs were examined for the
presence of sarcocysts. The prevalence rate was 67.98%, of which 43.14% wasSarcocystis miescheriana and 47.11% was S. suihominis (Saleque and Bhatia, 1991).
The prevalence of Sarcocystis in muscle of 36 caribou examined in Newfound-
land, Canada, was 53%. Infected animals were more frequently found in the centralpart of the island (Khan and Fong, 1991).
In Ethiopia, Sarcocystis was identified in 93% of sheep, 82% of cattle, 81% of
goats, 16.6% of donkeys, and 6.6% of chickens, from a total of 671 animals. Noneof the 40 heart muscles from bovine, ovine, caprine, and donkey fetuses examinedharbored Sarcocystis (Woldemeskel and Gebreab, 1996).
In Fars Province of Iran, 786 (57.7%) of 1362 animals examined were pos-
itive for Sarcocystis. The prevalence was significantly higher ( p < 0.05) in ani-mals owned by nomadic Assyrians (67.95%) than in those owned by local people(41.86%). Animals older than 2 years of age (69.98%) were more infected com-pared to young ones (30.02%). Sarcocystis gigantea was predominantly identifiedin the oesophagus, Sarcocystis medusiformis mainly in the diaphragm, S. tenellain the oesophagus, diaphragm, tongue, and heart, and Sarcocystis arieticanis in theoesophagus, tongue, and occasionally in the diaphragm (Oryan et al., 1996).
In Japan,S. suihominis was detected for the first time in the heart and diaphragm
of 5 out of 600 older culled breeding pigs slaughtered in the Saitama Prefecture(Saito et al., 1998).
A survey was carried out to investigate the occurrence of Sarcocystis infection
in the loin of 482 Japanese and imported beef. The prevalence of Sarcocystis waslower in Japanese beef (total 6.31%: 0% in Holstein castrated, 12.96% in Holsteinmilk cow, 3.33% in Japanese shorthorn, and 11.58% in Japanese black cattle) thanin beef imported from America (36.78%) or Australia (29.49%). All detected cystsexcept one were identified as S. cruzi. One thick walled cyst was found in Australianbeef, but it could not be distinguished as either S. hirsuta or S. hominis (Ono andOhsumi, 1999).
In the Upper East Region (UER) of Ghana a cross-sectional study was carried
out to estimate the prevalence of parasitic infections in local cross-bred pigs. Tenout of 60 villages with a human population of 200–1000 inhabitants were randomlyselected for the study. The number of pigs varied from 50 to 200 pigs per village. Sarcocystis sp. was observed in 28.3% animals (Permin et al., 1999).
A survey of Sarcocystis infection was conducted in Mongolia between June
1998 and July 1999. The prevalence of infection was cattle 90.0% (27/30), yak93.3% (28/30), hainag 100% (30/30), sheep 96.9% (753/777), horses 75% (3/4),and camels 100% (5/5). Heart was most commonly infected in cattle (100%), yak
Figure 3.1. Isospora (a) modified acid-fast stain, (b, c) unsporulated and sporulated oocyst, (d) autofluorescence. Cyclospora oocysts (e) modified acid-fast stain, (f, g) unsporulated oocyst, and (g) autofluorescence.
(86.7%), and hainag (100%); tongue was most commonly infected in sheep (100%)and horses (100%) (Fukuyo et al., 2002).
Domestic animals have also been reported harboring Sarcocystis. In Rio de
Janeiro, Brazil, 0.8% of fecal samples had Sarcocystis sp. in a survey of 131 domes-ticated and stray cats (Serra et al., 2003). 3.6 DIAGNOSIS
Diagnosis of these parasites is done by the identification of the oocysts or sporocystsin the fecal samples of the infected individuals. Oocysts can be observed using phasecontrast or bright field or DIC microscopy (Fig. 3.1). Cyclospora and Isosporaoocysts and Sarcocystis sporocysts autofluoresce; therefore, a fecal suspension isobserved using a epifuorescence microscope with an excytation filter of 360/40 nm,a long pass dichroic mirror of 400 nm and a 420 nm emission filter (Fig. 3.1)(Lindquist et al., 2003). A Kinyoun, Ziehl Nielsen, or carbolfucsin modified acidfast stain can be used to stain oocysts, however Cyclospora oocysts take the stainvariably; therefore, if a sample contains a low number of oocysts they could bemissed. A safranin stain has also been reported (Fig. 3.1). This stain works betterthan the previously described because oocysts stain bright pink and most oocyststake the stain (Visvesvara et al., 1997).
These procedures are not very practical when examining environmental samples,
because oocysts are usually in small numbers and many structures may look alike. It is then recommended to use molecular tools to identify these parasites.
In 1996, a PCR assay for Cyclospora was developed using clinical samples
(Relman et al., 1996). It was later determined that this PCR, although sensitive,was not specific for Cyclospora. When working with environmental samples, othercoccidian parasites noninfectious to humans were also amplifying a product ofthe same size as Cyclospora. Jineman then developed a PCR-RFLP which could
differentiate among these coccidia (Jinneman et al., 1998). This was followed bynew strategies to develop more sensitive and specific assays. These included theoligonucleotide-ligation assay (OLA) (Jinneman et al., 1999) and real-time PCR(Varma et al., 2003). The sensitivity of these assays could be improved by optimizingthe DNA extraction procedures and eliminating PCR inhibitors. Some of thesestrategies included the use of FTA filters (Orlandi and Lampel, 2000) and inclusionof resin matrix treatment during oocyst disruption (Jinneman et al., 1998). PCRamplification of the Isospora SSU-rRNA gene has also been described Li et al.,2002; Muller et al., 2000; Yang et al., 2002). Sarcocystis hirsuta isolates from cattle, Sarcocystis hominis-like isolates and a
Sarcocystis cruzi isolate were examined by PCR amplification of the 18S rRNADNA. These species could be fast and easily differentiated by sequencing of theamplified products and PCR-RFLP (Fischer and Odening, 1998; Yang et al., 2002).
An IFA-test (Indirect Fluorescent Antibody Test) for the diagnosis of sarcocys-
tosis in the intermediate host was identified in mice inoculated experimentally withSarcocystis dispersa; however, cross reaction was observed with Frenkelia (Cernaand Kolarova, 1978). Habeeb studied the humoral response in patients with idio-pathic cardiac diseases and rheumatic diseases. The enzyme-linked immunosorbentassay (ELISA) and indirect fluorescent antibody technique (IFAT) using Sarcocystisfusiformis antigen could specifically identify cases with Sarcocystis and idiopathiccardiac diseases (Cerna and Kolarova, 1978; Habeeb et al., 1996).
Histopathological descriptions of these infections have been reported. Micro-
scopic examination of the excised tissue of cases that presented with lumps, pain inthe limbs, or a discharging sinus showed characteristic cysts of Sarcocystis (Mehrotraet al., 1996). Parasitic vacuoles of patients with cyclosporiasis were observed morecommonly in individuals that were immunocompromised. Immunocompetent in-dividuals rarely presented parasitic vacuoles; however, the epithelial disarray andinflammation was consistently present (Ortega et al., 1997a). Isospora intracellularstages have been observed in intestinal biopsies of infected individuals, particularlyin AIDS patients. 3.7 TREATMENT AND CONTROL
Treatment of choice for cyclosporiasis is trimethoprim sulfamethoxazole (TMP-SMX) (Madico et al., 1993; Pape et al., 1994). In a randomized control trial,ciprofloxacin was suggested as an alternative treatment for patients with cyclospo-riasis who are allergic to sulfa drugs (Verdier et al., 2000).
Trimethoprim sulfamethoxazole (TMP/SMX) is the drug of choice for treat-
ment of isosporiasis. However, patients allergic or intolerant to TMP/SMX maytake Ciprofloxacine as an alternative treatment. (Verdier et al., 2000). Patientswith AIDS have a high rate of adverse reactions to this therapy. Two patientswith AIDS and isosporiasis that were sulfonamide allergic were treated success-fully with pyrimethamine alone, 75 mg/d, and recurrence was prevented with dailypyrimethamine therapy, 25 mg/d (Weiss et al., 1988). Doxycycline and nifuroxazide
has also been studied in AIDS patients. Relapsed Isospora infections were long-termtreated with doxycycline (Meyohas et al., 1990). Sarcocystis infections in humans responded to a one month treatment with sul-
fadiazine or finidazole (Yu, 1991).
Because the mechanisms of transmission of Cyclospora and Isospora are as-
sociated with the consumption of contaminated water or foods, control of theseinfections can be achieved by avoiding fresh produce in areas of endemnicity anddrinking purified water (by filtration or boiling). Since Cyclospora is highly resis-tant to chlorination, this procedure should not be considered as an alternative watertreatment. Sarcocystis infections can be prevented by eating well-cooked meats,particularly game meats, and pork (Yu, 1991).
The methods currently used in the sanitation of fresh food products are ineffec-
tive against Cyclospora, Isospora and Sarcocystis. These parasites are particularlyresistant to sanitizers and disinfectants. Therefore, prevention is the best strategyto reduce the risk of infections and can be accomplished by the implementation ofgood agricultural practices during all stages of production, harvesting and commer-cialization. REFERENCES
Anonymous, 2004, Outbreak of cyclosporiasis associated with snow peas—Pennsylvania,
2004, Morb. Mortal. Wkly. Rep. 53: 876–878.
Alakpa, G., Fagbenro-Beyioku, A. F., and Clarke, S. C., 2002, Cyclospora cayetanensis in
stools submitted to hospitals in Lagos, Nigeria, Int. J. Infect. Dis. 6:314–318.
Alakpa, G. E., Clarke, S. C., and Fagbenro-Beyioku, A. F., 2003, Cyclospora cayetanensis
infection in Lagos, Nigeria, Clin. Microbiol. Infect. 9:731–733.
Ali, M. S., Mahmoud, L. A., Abaza, B. E., and Ramadan, M. A., 2000, Intestinal spore-forming
protozoa among patients suffering from chronic renal failure, J. Egypt. Soc. Parasitol. 30:93–100.
Arnaud-Battandier, F., 1985, Cryptosporidiosis, isosporiasis, lambliasis in immunologic de-
ficiencies, Arch. Fr. Pediatr. 42(Suppl 2):959–963.
Ashford, R. W., 1979, Occurrence of an undescribed coccidian in man in Papua New Guinea,
Ann. Trop. Med. Parasitol. 73:497–500.
Azab, M. E., and el-Shennawy, S. F., 1992, Investigation of Sarcocystis as a causative agent
in cardiac disease, J. Egypt. Soc. Parasitol. 22:611–616.
Beaver, P. C., Gadgil, K., and Morera, P., 1979, Sarcocystis in man: A review and report of
five cases, Am. J. Trop. Med. Hyg. 28:819–844.
Beck, J. W., Stanton, R. L., and Langford, G. C., Jr., 1955, Human infection with Isosporabelli; report of a case in Florida, Am. J. Clin. Pathol. 25:648–651.
Bern, C., Hernandez, B., Lopez, M. B., Arrowood, M. J., de Merida, A. M., and Klein,
R. E., 2000, The contrasting epidemiology of Cyclospora and Cryptosporidium among outpatients in Guatemala, Am. J. Trop. Med. Hyg. 63:231–235.
Bern, C., Ortega, Y., Checkley, W., Roberts, J. M., Lescano, A. G., Cabrera, L., Verastegui,
M., Black, R. E., Sterling, C., and Gilman, R. H., 2002, Epidemiologic differences between cyclosporiasis and cryptosporidiosis in Peruvian children, Emerg. Infect. Dis. 8:581–585.
Bottner, A., Charleston, W. A., Pomroy, W. E., and Rommel, M., 1987, The prevalence and
identity of Sarcocystis in beef cattle in New Zealand, Vet. Parasitol. 24:157–168.
Brandonisio, O., Maggi, P., Panaro, M. A., Lisi, S., Andriola, A., Acquafredda, A., and
Angarano, G., 1999, Intestinal protozoa in HIV-infected patients in Apulia, South Italy, Epidemiol. Infect. 123:457–462.
Brantley, R. K., Williams, K. R., Silva, T. M., Sistrom, M., Thielman, N. M., Ward, H., Lima,
A. A., and Guerrant, R. L., 2003, AIDS-associated diarrhea and wasting in Northeast Brazil is associated with subtherapeutic plasma levels of antiretroviral medications and with both bovine and human subtypes of Cryptosporidium parvum, Braz. J. Infect. Dis. 7:16–22.
Bunyaratvej, S., and Unpunyo, P., 1992, Combined Sarcocystis and gram-positive bacterial
infections. A possible cause of segmental enterocolitis in Thailand, J. Med. Assoc. Thai. 75(Suppl 1):38–44.
Bunyaratvej, S., Bunyawongwiroj, P., and Nitiyanant, P., 1982, Human intestinal sarcosporid-
iosis: Report of six cases, Am. J. Trop. Med. Hyg. 31:36–41.
Caceres, V. M., Ball, R. T., Somerfeldt, S. A., Mackey, R. L., Nichols, S. E., MacKenzie, W.
R., and Herwaldt, B. L., 1998, A foodborne outbreak of cyclosporiasis caused by imported raspberries, J. Fam. Pract. 47:231–234.
Carollo, M. C., Amato Neto, V., Braz, L. M., and Kim, D. W., 2001, Detection of Cyclospora
sp. oocysts in the feces of stray dogs in Greater Sao Paulo (Sao Paulo State, Brazil), Rev. Soc. Bras. Med. Trop. 34:597–598.
Cegielski, J. P., Ortega, Y. R., McKee, S., Madden, J. F., Gaido, L., Schwartz, D. A., Manji, K.,
Jorgensen, A. F., Miller, S. E., Pulipaka, U. P., Msengi, A. E., Mwakyusa, D. H., Sterling, C. R., and Reller, L. B., 1999, Cryptosporidium, enterocytozoon, and cyclospora infections in pediatric and adult patients with diarrhea in Tanzania, Clin. Infect. Dis. 28:314–321.
Cerna, Z., and Kolarova, I., 1978, Contribution to the serological diagnosis of sarcocystosis,
Folia Parasitol. (Praha) 25:289–292.
Chacin-Bonilla, L., Estevez, J., Monsalve, F., and Quijada, L., 2001, Cyclospora cayetanensis
infections among diarrheal patients from Venezuela, Am. J. Trop. Med. Hyg. 65:351–354.
Chacin-Bonilla, L., Mejia de Young, M., and Estevez, J., 2003, Prevalence and pathogenic
role of Cyclospora cayetanensis in a Venezuelan community, Am. J. Trop. Med. Hyg. 68:304–306.
Charatan, F. B., 1996, Cyclospora outbreak in US, BMJ 313:71. Chen, X., Zuo, Y., and Zuo, W., 1999, Observation on the clinical symptoms and sporocyst
excretion in human volunteers experimentally infected with Sarcocystis hominis, Zhongguo Ji Sheng Chong Xue Yu Ji Sheng Chong Bing Za Zhi 17:25–27.
Chu, D. M., Sherchand, J. B., Cross, J. H., and Orlandi, P. A., 2004, Detection of Cyclosporacayetanensis in animal fecal isolates from Nepal using an FTA filter-base polymerase chain reaction method, Am. J. Trop. Med. Hyg. 71:373–379.
Cimerman, S., Cimerman, B., and Lewi, D. S., 1999, Prevalence of intestinal parasitic infec-
tions in patients with acquired immunodeficiency syndrome in Brazil, Int. J. Infect. Dis. 3:203–206.
Connor, B. A., and Shlim, D. R., 1995, Foodborne transmission of Cyclospora, Lancet346:1634.
Cranendonk, R. J., Kodde, C. J., Chipeta, D., Zijlstra, E. E., and Sluiters, J. F., 2003, Cryp-tosporidium parvum and Isospora belli infections among patients with and without diar- rhoea, East Afr. Med. J. 80:398–401.
Dionisio, D., Santucci, M., Comin, C. E., Di Lollo, S., Orsi, A., Gabbrielli, M., Milo, D.,
Rogasi, P. G., Meli, M., and Vigano, S., 1992, Isosporiasis and sarcocystosis: The current findings, Recenti. Prog. Med. 83:719–725.
Dissanaike, A. S., 1994, Human Sarcocystis infection, Trans. R. Soc. Trop. Med. Hyg. 88:364. Doller, P. C., Dietrich, K., Filipp, N., Brockmann, S., Dreweck, C., Vonthein, R., Wagner-
Wiening, C., and Wiedenmann, A., 2002, Cyclosporiasis outbreak in Germany associated with the consumption of salad, Emerg. Infect. Dis. 8:992–994.
Dowd, S. E., John, D., Eliopolus, J., Gerba, C. P., Naranjo, J., Klein, R., Lopez, B., de
Mejia, M., Mendoza, C. E., and Pepper, I. L., 2003, Confirmed detection of Cyclospora cayetanesis, Encephalitozoon intestinalis and Cryptosporidium parvum in water used for drinking, J. Water Health 1:117–123.
Drenaggi, D., Cirioni, O., Giacometti, A., Fiorentini, A., and Scalise, G., 1998, Cyclosporiasis
in a traveler returning from South America, J. Travel Med. 5:153–155.
Dubey, J. P., 1976, A review of Sarcocystis of domestic animals and of other coccidia of cats
and dogs, J. Am. Vet. Med. Assoc. 169:1061–1078.
Dubey, J. P., 1993, Toxoplasma, Neospora, Sarcocystis, and other Tissue Cyst-Forming Coc-
cidia of Humans and Animals. In Kreier, J. P. and Baker, J. R. (eds), Pathogenic Protozoa,Academic Press, Inc., San Diego, California, pp. 1–156.
Eberhard, M. L., Ortega, Y. R., Hanes, D. E., Nace, E. K., Do, R. Q., Robl, M. G., Won, K. Y.,
Gavidia, C., Sass, N. L., Mansfield, K., Gozalo, A., Griffiths, J., Gilman, R., Sterling, C. R., and Arrowood, M. J., 2000, Attempts to establish experimental Cyclospora cayetanensis infection in laboratory animals, J. Parasitol. 86:577–582.
Eberhard, M. L., Njenga, M. N., DaSilva, A. J., Owino, D., Nace, E. K., Won, K. Y., and
Mwenda, J. M., 2001, A survey for Cyclospora spp. in Kenyan primates, with some notes on its biology, J. Parasitol. 87:1394–1397.
Fayer, R., 2004, Sarcocystis spp. in human infections, Clin. Microbiol. Rev. 17:894–902. Fayer, R., Heydorn, A. O., Johnson, A. J., and Leek, R. G., 1979, Transmission of Sarcocystis suihominis from humans to swine to nonhuman primates (Pan troglodytes, Macaca mulatta, Macaca irus), Z. Parasitenkd. 59:15–20.
Ferreira, L. F., Coutinho, S. G., Argento, C. A., and da, S. J., 1962, Experimental human
coccidial enteritis by Isospora belli Wenyon, 1923: A study based on the infection of 5 volunteers, Hospital (Rio J) 62:795–804.
Ferreira, M. S., 2000, Infections by protozoa in immunocompromised hosts, Mem. Inst.Oswaldo Cruz 95(Suppl 1):159–162.
Figueroa, F., Palacios, A., Rivero, S., Oddo, D., Roa, I., Honeyman, J., Gatica, M. A., and
Acuna, G., 1985, Chronic diarrhea due to Isospora belli and Kaposi’s sarcoma in a male homosexual. Report of the 1st case of acquired immunodeficiency syndrome in Chile, Rev. Med. Chil. 113:772–779.
Fischer, S., and Odening, K., 1998, Characterization of bovine Sarcocystis species by analysis
of their 18S ribosomal DNA sequences, J. Parasitol. 84:50–54.
Fleming, C. A., Caron, D., Gunn, J. E., and Barry, M. A., 1998, A foodborne outbreak of
Cyclospora cayetanensis at a wedding: Clinical features and risk factors for illness, Arch. Intern. Med. 158:1121–1125.
Frenkel, J. K., Heydorn, A. O., Mehlhorn, H., and Rommel, M., 1979, Sarcocystinae: Nomina
dubia and available names, Z. Parasitenkd. 58:115–139.
Fukuyo, M., Battsetseg, G., and Byambaa, B., 2002, Prevalence of Sarcocystis infection
in meat-producing animals in Mongolia, Southeast Asian J. Trop. Med. Public Health 33:490–495.
Furio, M. M., and Wordell, C. J., 1985, Treatment of infectious complications of acquired
immunodeficiency syndrome, Clin. Pharm. 4:539–554.
Garcia-Lopez, H. L., Rodriguez-Tovar, L. E., and Medina-De la Garza, C. E., 1996, Identifi-
cation of Cyclospora in poultry, Emerg. Infect. Dis. 2:356–357.
Gascon, J., Corachan, M., Bombi, J. A., Valls, M. E., and Bordes, J. M., 1995, Cyclospora
in patients with traveller’s diarrhea, Scand. J. Infect. Dis. 27:511–514.
Gassama, A., Sow, P. S., Fall, F., Camara, P., Gueye-N’diaye, A., Seng, R., Samb, B., M’Boup,
S., and Aidara-Kane, A., 2001, Ordinary and opportunistic enteropathogens associated with diarrhea in Senegalese adults in relation to human immunodeficiency virus serostatus, Int. J. Infect. Dis. 5:192–198.
Gut, J., 1982, Effectiveness of methods used for the detection of sarcosporidiosis in farm
animals, Folia Parasitol. (Praha) 29:289–295.
Habeeb, Y. S., Selim, M. A., Ali, M. S., Mahmoud, L. A., Abdel Hadi, A. M., and Shafei,
A., 1996, Serological diagnosis of extraintestinal Sarcocystosis, J. Egypt. Soc. Parasitol. 26:393–400.
Henry, M. C., De Clercq, D., Lokombe, B., Kayembe, K., Kapita, B., Mamba, K., Mbendi,
N., and Mazebo, P., 1986, Parasitological observations of chronic diarrhoea in suspected AIDS adult patients in Kinshasa (Zaire), Trans. R. Soc. Trop. Med. Hyg. 80:309–310.
Herwaldt, B. L., 2000, Cyclospora cayetanensis: A review, focusing on the outbreaks of
cyclosporiasis in the 1990s, Clin. Infect. Dis. 31:1040–1057.
Herwaldt, B. L., and Ackers, M. L., 1997, An outbreak in 1996 of cyclosporiasis associated
with imported raspberries. The Cyclospora Working Group, N. Engl. J. Med. 336:1548– 1556.
Herwaldt, B. L., and Beach, M. J., 1999, The return of Cyclospora in 1997: Another out-
break of cyclosporiasis in North America associated with imported raspberries. Cyclospora Working Group, Ann. Intern. Med. 130:210–220.
Heydorn, A. O., 1977, Life-cycle of Sarcosporidia. IX. Developmental cyclus of Sarcocystissuihominis n. spec., Berl. Munch. Tierarztl. Wochenschr. 90:218–224.
Heydorn, A. O., Mehlhorn, H., and Gestrich, R., 1975, Light and electron microscopic studies
on cysts of Sarcocystis fusiformis in the muscles of calves infected experimentally with oocytes and sporocysts of the large form of Isospora bigemina from dogs. 2. The fine structure of cyst stages., Zentralbl. Bakteriol. [Orig A] 233:123–137.
Hoge, C. W., Shlim, D. R., Rajah, R., Triplett, J., Shear, M., Rabold, J. G., and Echeverria, P.,
1993, Epidemiology of diarrhoeal illness associated with coccidian-like organism among travellers and foreign residents in Nepal, Lancet 341:1175–1179.
Hoge, C. W., Echeverria, P., Rajah, R., Jacobs, J., Malthouse, S., Chapman, E., Jimenez, L.
M., and Shlim, D. R., 1995, Prevalence of Cyclospora species and other enteric pathogens among children less than 5 years of age in Nepal, J. Clin. Microbiol. 33:3058–3060.
Huang, P., Weber, J. T., Sosin, D. M., Griffin, P. M., Long, E. G., Murphy, J. J., Kocka, F.,
Peters, C., and Kallick, C., 1995, The first reported outbreak of diarrheal illness associated with Cyclospora in the United States, Ann. Intern. Med. 123:409–414.
Jelinek, T., Lotze, M., Eichenlaub, S., Loscher, T., and Nothdurft, H. D., 1997, Prevalence of
infection with Cryptosporidium parvum and Cyclospora cayetanensis among international travellers, Gut 41:801–804.
Jinneman, K. C., Wetherington, J. H., Hill, W. E., Adams, A. M., Johnson, J. M., Tenge,
B. J., Dang, N. L., Manger, R. L., and Wekell, M. M., 1998, Template preparation for PCR and RFLP of amplification products for the detection and identification of Cy- clospora sp. and Eimeria spp. Oocysts directly from raspberries, J. Food Prot. 61:1497– 1503.
Jinneman, K. C., Wetherington, J. H., Hill, W. E., Omiescinski, C. J., Adams, A. M., Johnson, J.
M., Tenge, B. J., Dang, N. L., and Wekell, M. M., 1999, An oligonucleotide-ligation assay for the differentiation between Cyclospora and Eimeria spp. polymerase chain reaction amplification products, J. Food Prot. 62:682–685.
Jonas, C., Van de Perre, P., Reding, P., Burette, A., Deprez, C., Clumeck, N., and Deltenre,
M., 1984, Severe digestive complications of AIDS in a group of patients from Zaire, Acta Gastroenterol. Belg. 47:396–402.
Joshi, M., Chowdhary, A. S., Dalal, P. J., and Maniar, J. K., 2002, Parasitic diarrhoea in
patients with AIDS, Natl. Med. J. India 15:72–74.
Kan, S. P., and Pathmanathan, R., 1991, Review of sarcocystosis in Malaysia, Southeast AsianJ. Trop. Med. Public Health 22 (Suppl):129–134.
Katz, D., Kumar, S., Malecki, J., Lowdermilk, M., Koumans, E. H., and Hopkins, R., 1999,
Cyclosporiasis associated with imported raspberries, Florida, 1996, Public Health Rep. 114:427–438.
Khan, R. A., and Fong, D., 1991, Sarcocystis in caribou (Rangifer tarandus terraenorae) in
Newfoundland, Southeast Asian J. Trop. Med. Public Health 22(Suppl):142–143.
Kimmig, P., Piekarski, G., and Heydorn, A. O., 1979, Sarcosporidiosis (Sarcocystis suihomi-nis) in man (author’s transl), Immun. Infekt. 7:170–177.
Kobayashi, L. M., Kort, M. P., Berlin, O. G., and Bruckner, D. A., 1985, Isospora infection
in a homosexual man, Diagn. Microbiol. Infect. Dis. 3:363–366.
Kutty, M. K., and Dissanaike, A. S., 1975, A case of human Sarcocystis infection in west
Malaysia, Trans. R. Soc. Trop. Med. Hyg. 69:503–504.
Lainson, R., and da Silva, B. A., 1999, Intestinal parasites of some diarrhoeic HIV-seropositive
individuals in North Brazil, with particular reference to Isospora belli Wenyon, 1923 and Dientamoeba fragilis Jepps & Dobell, 1918, Mem. Inst. Oswaldo Cruz 94:611–613.
Lebbad, M., Norrgren, H., Naucler, A., Dias, F., Andersson, S., and Linder, E., 2001, Intestinal
parasites in HIV-2 associated AIDS cases with chronic diarrhoea in Guinea-Bissau, Acta. Trop. 80:45–49.
Li, Q. Q., Yang, Z. Q., Zuo, Y. X., Attwood, S. W., Chen, X. W., and Zhang, Y. P., 2002,
A PCR-based RFLP analysis of Sarcocystis cruzi (Protozoa: Sarcocystidae) in Yunnan Province, PR China, reveals the water buffalo (Bubalus bubalis) as a natural intermediate host, J. Parasitol. 88:1259–1261.
Lian, Z., Ma, J., Wang, Z., Fu, L., Zhou, Z., Li, W., and Wang, X., 1990, Studies on man-
cattle-man infection cycle of Sarcocystis hominis in Yunnan, Zhongguo Ji Sheng Chong Xue Yu Ji Sheng Chong Bing Za Zhi 8:50–53.
Lindquist, H. D., Bennett, J. W., Hester, J. D., Ware, M. W., Dubey, J. P., and Everson, W. V.,
2003, Autofluorescence of Toxoplasma gondii and related coccidian oocysts, J. Parasitol. 89:865–867.
Lindsay, S. S., Dubey, J. P., and Blagburn, B. L., 1997, Biology of Isospora spp. from humans,
nonhuman primates and domestic animals, Clin. Microb. Rev. 10:19–34.
Long, E. G., White, E. H., Carmichael, W. W., Quinlisk, P. M., Raja, R., Swisher, B. L.,
Daugharty, H., and Cohen, M. T., 1991, Morphologic and staining characteristics of a cyanobacterium-like organism associated with diarrhea, J. Infect. Dis. 164:199–202.
Lopez, A. S., Dodson, D. R., Arrowood, M. J., Orlandi Jr, P. A., da Silva, A. J., Bier, J.
W., Hanauer, S. D., Kuster, R. L., Oltman, S., Baldwin, M. S., Won, K. Y., Nace, E. M., Eberhard, M. L., and Herwaldt, B. L., 2001, Outbreak of cyclosporiasis associated with basil in Missouri in 1999, Clin. Infect. Dis. 32:1010–1017.
Lopez, A. S., Bendik, J. M., Alliance, J. Y., Roberts, J. M., da Silva, A. J., Moura, I. N.,
Arrowood, M. J., Eberhard, M. L., and Herwaldt, B. L., 2003, Epidemiology of Cyclospora cayetanensis and other intestinal parasites in a community in Haiti, J. Clin. Microbiol. 41:2047–2054.
Ma, P., Kaufman, D., and Montana, J., 1983, Isospora belli diarrheal infection in homosexual
men, AIDS Res. 1:327–338.
Madico, G., Gilman, R. H., Miranda, E., Cabrera, L., and Sterling, C. R., 1993, Treatment of
Cyclospora infections with co-trimoxazole, Lancet 342:122–123.
Madico, G., McDonald, J., Gilman, R. H., Cabrera, L., and Sterling, C. R., 1997, Epidemiology
and treatment of Cyclospora cayetanensis infection in Peruvian children, Clin. Infect. Dis. 24:977–981.
Maiga, M. Y., Dembele, M. Y., Traore, H. A., Kouyate, M., Traore, A. K., Maiga, I.,
Bougoudogo, F., Doumbo, O., and Guindo, A., 2002, Gastrointestinal manifestations of AIDS in adults in Mali, Bull. Soc. Pathol. Exot. 95:253–256.
Makni, F., Cheikrouhou, F., and Ayadi, A., 2000, Parasitoses and immunodepression, Arch.Inst. Pasteur. Tunis. 77:51–54.
Mansfield, L. S., and Gajadhar, A. A., 2004, Cyclospora cayetanensis, a food- and waterborne
coccidian parasite, Vet. Parasitol. 126:73–90.
Markus, M. B., and Frean, J. A., 1993, Occurrence of human Cyclospora infection in sub-
Saharan Africa, S. Afr. Med. J. 83:862–863.
McLeod, R., Hirabayashi, R. N., Rothman, W., and Remington, J. S., 1980, Necrotizing
vasculitis and Sarcocystis: A cause-and-effect relationship? South. Med. J. 73:1380–1383.
Mehrotra, R., Bisht, D., Singh, P. A., Gupta, S. C., and Gupta, R. K., 1996, Diagnosis
of human sarcocystis infection from biopsies of the skeletal muscle, Pathology 28:281– 282.
Meyohas, M. C., Capella, F., Poirot, J. L., Lecomte, I., Binet, D., Eliaszewicz, M., and Frottier,
J., 1990, Treatment with doxycycline and nifuroxazide of Isospora belli infection in AIDS, Pathol. Biol. (Paris) 38:589–591.
Modigliani, R., Bories, C., Le Charpentier, Y., Salmeron, M., Messing, B., Galian, A.,
Rambaud, J. C., Lavergne, A., Cochand-Priollet, B., and Desportes, I., 1985, Diarrhoea and malabsorption in acquired immune deficiency syndrome: A study of four cases with special emphasis on opportunistic protozoan infestations, Gut 26:179–187.
Mohandas, S., R., Sud, A., and Malla, N., 2002, Prevalence of intestinal parasitic pathogens
in HIV-seropositive individuals in Northern India, Jpn J. Infect. Dis. 55:83–84.
Muller, A., Bialek, R., Fatkenheuer, G., Salzberger, B., Diehl, V., and Franzen, C., 2000,
Detection of Isospora belli by polymerase chain reaction using primers based on small- subunit ribosomal RNA sequences, Eur. J. Clin. Microbiol. Infect. Dis. 19:631–634.
Ng, E., Markell, E. K., Fleming, R. L., and Fried, M., 1984, Demonstration of Isosporabelli by acid-fast stain in a patient with acquired immune deficiency syndrome, J. Clin. Microbiol. 20:384–386.
Obana, M., Sagara, H., Aoki, T., Kim, R., Takizawa, Y., Tsunoda, T., Irimajiri, S., and
Yamashita, K., 2002, The current status of infectious enteritis in Japan—reports of the “Research Group for Infectious Enteric Diseases, Japan” in the last 5 years (1996–2000), Kansenshogaku Zasshi 76:355–368.
Ono, M., and Ohsumi, T., 1999, Prevalence of Sarcocystis spp. cysts in Japanese and imported
beef (Loin: Musculus longissimus), Parasitol. Int. 48:91–94.
Orlandi, P. A., and Lampel, K. A., 2000, Extraction-free, filter-based template preparation
for rapid and sensitive PCR detection of pathogenic parasitic protozoa, J. Clin. Microbiol. 38:2271–2277.
Ortega, Y. R., Sterling, C. R., Gilman, R. H., Cama, V. A., and Diaz, F., 1993, Cyclospora
species–a new protozoan pathogen of humans, N. Engl. J. Med. 328:1308–1312.
Ortega, Y. R., Gilman, R. H., and Sterling, C. R., 1994, A new coccidian parasite (Apicom-
plexa: Eimeriidae) from humans, J. Parasitol. 80:625–629.
Ortega, Y. R., Nagle, R., Gilman, R. H., Watanabe, J., Miyagui, J., Quispe, H., Kanagusuku,
P., Roxas, C., and Sterling, C. R., 1997a, Pathologic and clinical findings in patients with cyclosporiasis and a description of intracellular parasite life-cycle stages, J. Infect. Dis. 176:1584–1589.
Ortega, Y. R., Roxas, C. R., Gilman, R. H., Miller, N. J., Cabrera, L., Taquiri, C., and
Sterling, C. R., 1997b, Isolation of Cryptosporidium parvum and Cyclospora cayetanensis from vegetables collected in markets of an endemic region in Peru, Am. J. Trop. Med. Hyg. 57:683–686.
Oryan, A., Moghaddar, N., and Gaur, S. N., 1996, The distribution pattern of Sarcocystis
species, their transmission and pathogenesis in sheep in Fars Province of Iran, Vet. Res. Commun. 20:243–253.
Pamphlett, R., and O’Donoghue, P., 1990, Sarcocystis infection of human muscle, Aust. N.Z. J. Med. 20:705–707.
Pamphlett, R., and O’Donoghue, P., 1992, Antibodies against Sarcocystis and Toxoplasma in
humans with the chronic fatigue syndrome, Aust. N. Z. J. Med. 22:307–308.
Panosian, C. B., 1988, Parasitic diarrhea, Infect. Dis. Clin. North. Am. 2:685–703. Pape, J. W., Verdier, R. I., Boncy, M., Boncy, J., and Johnson, W. D., Jr., 1994, Cyclospora
infection in adults infected with HIV. Clinical manifestations, treatment, and prophylaxis, Ann. Intern. Med. 121:654–657.
Pathmanathan, R., and Kan, S. P., 1992, Three cases of human Sarcocystis infection with
a review of human muscular sarcocystosis in Malaysia, Trop. Geogr. Med. 44:102– 108.
Pena, H. F., Ogassawara, S., and Sinhorini, I. L., 2001, Occurrence of cattle Sarcocystis
species in raw kibbe from Arabian food establishments in the city of Sao Paulo, Brazil, and experimental transmission to humans, J. Parasitol. 87:1459–1465.
Permin, A., Yelifari, L., Bloch, P., Steenhard, N., Hansen, N. P., and Nansen, P., 1999, Parasites
in cross-bred pigs in the Upper East region of Ghana, Vet. Parasitol. 87:63–71.
Piekarski, G., Heydorn, A. O., Aryeetey, M. E., Hartlapp, J. H., and Kimmig, P., 1978, Clinical,
parasitological and serological investigations in sarcosporidiosis (Sarcocystis suihominis) of man (author’s transl), Immun. Infekt. 6:153–159.
Pozio, E., 1991, Current status of food-borne parasitic zoonoses in Mediterranean and African
regions, Southeast Asian J. Trop. Med. Public Health 22(Suppl):85–87.
Pratdesaba, R. A., Gonzalez, M., Piedrasanta, E., Merida, C., Contreras, K., Vela, C., Culajay,
F., Flores, L., and Torres, O., 2001, Cyclospora cayetanensis in three populations at risk in Guatemala, J. Clin. Microbiol. 39:2951–2953.
Rabold, J. G., Hoge, C. W., Shlim, D. R., Kefford, C., Rajah, R., and Echeverria, P.,
1994, Cyclospora outbreak associated with chlorinated drinking water, Lancet 344:1360– 1361.
Relman, D. A., Schmidt, T. M., Gajadhar, A., Sogin, M., Cross, J., Yoder, K., Sethabutr,
O., and Echeverria, P., 1996, Molecular phylogenetic analysis of Cyclospora, the human intestinal pathogen, suggests that it is closely related to Eimeria species, J. Infect. Dis. 173:440–445.
Resiere, D., Vantelon, J. M., Bouree, P., Chachaty, E., Nitenberg, G., and Blot, F., 2003,
Isospora belli infection in a patient with non-Hodgkin’s lymphoma, Clin. Microbiol. Infect. 9:1065–1067.
Ribes, J. A., Seabolt, J. P., and Overman, S. B., 2004, Point prevalence of Cryptosporidium,
Cyclospora, and Isospora infections in patients being evaluated for diarrhea, Am. J. Clin. Pathol. 122:28–32.
Rizk, H., and Soliman, M., 2001, Coccidiosis among malnourished children in Mansoura,
Dakahlia Governorate, Egypt, J. Egypt. Soc. Parasitol. 31:877–886.
Rommel, M., and Heydorn, A. O., 1972, Contributions to the life cycle of Sarcosporidia.
3. Isospora hominis (Railliet and Lucet, 1891) Wenyon, 1923, the sporocyst of the Sar- cosporidia of cattle and swine, Berl Munch Tierarztl Wochenschr 85:143–145.
Ros, E., Fueyo, J., Llach, J., Moreno, A., and Latorre, X., 1987, Isospora belli infection in
patients with AIDS in Catalunya, Spain, N. Engl. J. Med. 317:246–247.
Sadaka, H. A., and Zoheir, M. A., 2001, Experimental studies on cyclosporiosis, J. Egypt.Soc. Parasitol. 31:65–77.
Saito, M., Shibata, Y., Ohno, A., Kubo, M., Shimura, K., and Itagaki, H., 1998, Sarcocystissuihominis detected for the first time from pigs in Japan, J. Vet. Med. Sci. 60:307–309.
Saleque, A., and Bhatia, B. B., 1991, Prevalence of Sarcocystis in domestic pigs in India, Vet.Parasitol. 40:151–153.
Serra, C. M., Uchoa, C. M., and Coimbra, R. A., 2003, Parasitological study with faecal
samples of stray and domiciliated cats (Felis catus domesticus) from the Metropolitan Area of Rio de Janeiro, Brazil, Rev. Soc. Bras. Med. Trop. 36:331–334.
Shein, R., and Gelb, A., 1984, Isospora belli in a patient with acquired immunodeficiency
syndrome, J. Clin. Gastroenterol. 6:525–528.
Sherchand, J. B., and Cross, J. H., 2001, Emerging pathogen Cyclospora cayetanensis infec-
tion in Nepal, Southeast Asian J. Trop. Med. Public Health 32(Suppl 2):143–150.
Shields, J. M., and Olson, B. H., 2003, PCR-restriction fragment length polymorphism method
for detection of Cyclospora cayetanensis in environmental waters without microscopic confirmation, Appl. Environ. Microbiol. 69:4662–4669.
Shlim, D. R., Hoge, C. W., Rajah, R., Scott, R. M., Pandy, P., and Echeverria, P., 1999,
Persistent high risk of diarrhea among foreigners in Nepal during the first 2 years of residence, Clin. Infect. Dis. 29:613–616.
Sivapalasingam, S., Friedman, C. R., Cohen, L., and Tauxe, R. V., 2004, Fresh produce: A
growing cause of outbreaks of foodborne illness in the United States, 1973 through 1997, J. Food Prot. 67:2342–2353.
Soave, R., 1988, Cryptosporidiosis and isosporiasis in patients with AIDS, Infect. Dis. Clin.North Am. 2:485–493.
Soave, R., Herwaldt, B. L., and Relman, D. A., 1998, Cyclospora, Infect. Dis. Clin. NorthAm. 12:1–12.
Straka, S., Skracikova, J., Konvit, I., Szilagyiova, M., and Michal, L., 1991, Sarcocystis
species in Vietnamese workers, Cesk. Epidemiol. Mikrobiol. Imunol. 40:204–208.
Tavarez, L. A., Pena, F., Placencia, F., Mendoza, H. R., and Polanco, D., 1991, Prevalence of
protozoans in children with acute diarrheal disease, Arch. Domin. Pediatr. 27:43–47.
Teschareon, S., Jariya, P., and Tipayadarapanich, C., 1983, Isospora belli infection as a cause
of diarrhoea, Southeast Asian J. Trop. Med. Public Health 14:528–530.
Uga, S., Kimura, D., Kimura, K., and Margono, S. S., 2002, Intestinal parasitic infections in
Bekasi district, West Java, Indonesia and a comparison of the infection rates determined by different techniques for fecal examination, Southeast Asian J. Trop. Med. Public Health 33:462–467.
Varma, M., Hester, J. D., Schaefer, F. W. 3rd, Ware, M. W., and Lindquist, H. D., 2003, De-
tection of Cyclospora cayetanensis using a quantitative real-time PCR assay, J. Microbiol. Methods 53:27–36.
Vercruysse, J., Fransen, J., and van Goubergen, M., 1989, The prevalence and identity of
Sarcocystis cysts in cattle in Belgium, Zentralbl Veterinarmed. B 36:148–153.
Verdier, R. I., Fitzgerald, D. W., Johnson, W. D., Jr., and Pape, J. W., 2000, Trimethoprim-
sulfamethoxazole compared with ciprofloxacin for treatment and prophylaxis of Isospora belli and Cyclospora cayetanensis infection in HIV-infected patients. A randomized, con- trolled trial, Ann. Intern. Med. 132:885–888.
Visvesvara, G. S., Moura, H., Kovacs-Nace, E., Wallace, S., and Eberhard, M. L., 1997,
Uniform staining of Cyclospora oocysts in fecal smears by a modified safranin technique with microwave heating, J. Clin. Microbiol. 35:730–733.
Weiss, L. M., Perlman, D. C., Sherman, J., Tanowitz, H., and Wittner, M., 1988, Isosporabelli infection: Treatment with pyrimethamine, Ann. Intern. Med. 109:474–475.
Whiteside, M. E., Barkin, J. S., May, R. G., Weiss, S. D., Fischl, M. A., and MacLeod, C. L.,
1984, Enteric coccidiosis among patients with the acquired immunodeficiency syndrome, Am. J. Trop. Med. Hyg. 33:1065–1072.
Wilairatana, P., Radomyos, P., Radomyos, B., Phraevanich, R., Plooksawasdi, W.,
Chanthavanich, P., Viravan, C., and Looareesuwan, S., 1996, Intestinal sarcocystosis in Thai laborers, Southeast Asian J. Trop. Med. Public Health 27:43–46.
Wiwanitkit, V., 2001, Intestinal parasitic infections in Thai HIV-infected patients with differ-
ent immunity status, BMC Gastroenterol. 1:3.
Woldemeskel, M., and Gebreab, F., 1996, Prevalence of sarcocysts in livestock of northwest
Ethiopia, Zentralbl Veterinarmed. B 43:55–58.
Wong, K. T., and Pathmanathan, R., 1992, High prevalence of human skeletal muscle sarco-
cystosis in south-east Asia, Trans. R. Soc. Trop. Med. Hyg. 86:631–632.
Wright, M. S., and Collins, P. A., 1997, Waterborne transmission of Cryptosporidium,
Cyclospora and Giardia, Clin. Lab. Sci. 10:287–290.
Yai, L. E., Bauab, A. R., Hirschfeld, M. P., de Oliveira, M. L., and Damaceno, J. T., 1997,
The first two cases of Cyclospora in dogs, Sao Paulo, Brazil, Rev. Inst. Med. Trop. Sao Paulo 39:177–179.
Yang, Z. Q., Li, Q. Q., Zuo, Y. X., Chen, X. W., Chen, Y. J., Nie, L., Wei, C. G., Zen, J.
S., Attwood, S. W., Zhang, X. Z., and Zhang, Y. P., 2002, Characterization of Sarcocystis species in domestic animals using a PCR-RFLP analysis of variation in the 18S rRNA gene: A cost-effective and simple technique for routine species identification, Exp. Parasitol. 102:212–217.
Yu, S., 1991, Field survey of sarcocystis infection in the Tibet autonomous region, ZhongguoYi Xue Ke Xue Yuan Xue Bao 13:29–32.
Zerpa, R., Uchima, N., and Huicho, L., 1995, Cyclospora cayetanensis associated with watery
diarrhoea in Peruvian patients, J. Trop. Med. Hyg. 98:325–329.
Zhang, B. X., Yu, H., Zhang, L. L., Tao, H., Li, Y. Z., Li, Y., Cao, Z. K., Bai, Z. M., and
He, Y. Q., 2002, Prevalence survey on Cyclospora cayetanensis and Cryptosporidium ssp. in diarrhea cases in Yunnan Province, Zhongguo Ji Sheng Chong Xue Yu Ji Sheng Chong Bing Za Zhi 20:106–108.
Patient Information Last, First MI (Preferred Name) Your Address: ______________________________________________________________________________ Street Apartment # City _________________________________ State/ZipCode ____________ EMAIL ADDRESS : ____________________ Social Security #: Birth Date: _________________ _ Family Status: ___________________ Phone (Home): Dentis
Quantitative LC-MS: “How Certain Can we be!”Peter Stokes, Gavin O’Connor, Chris Mussell, & Ken WebbLGC Limited, Queens Rd. Teddington, Middlesex, TW11 0LY. INTRODUCTION THE ANALYSIS OF CREATININE IN HUMAN SERUM CREATININE MEASUREMENTS USING DIFFERENT Less than 20% of all LC-MS publications involve MASS SPECTROMETRIC TECHNIQUES quantitation. The reasons for the slow
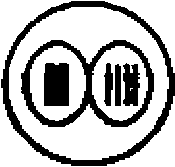
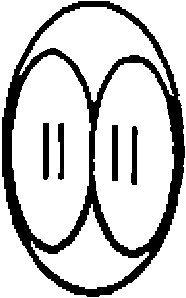
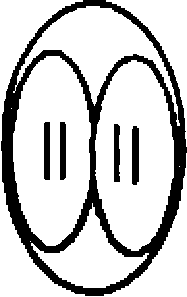 Table 3.1. Similarities and differences between Cyclospora, Sarcocystis, and Isospora
Table 3.1. Similarities and differences between Cyclospora, Sarcocystis, and Isospora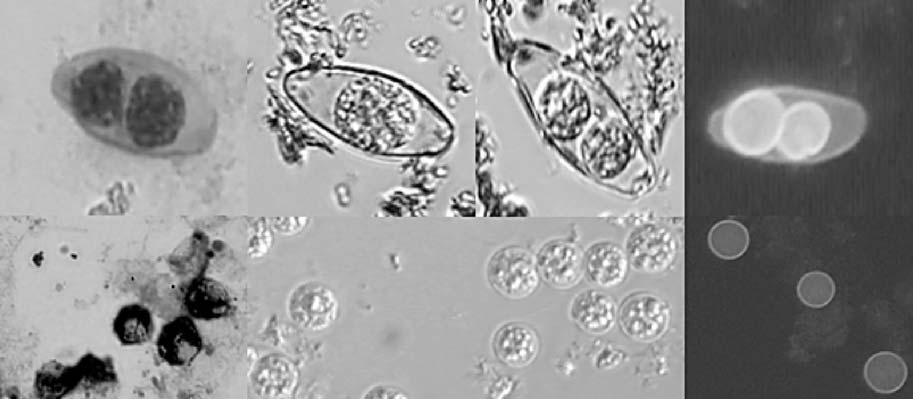 Figure 3.1. Isospora (a) modified acid-fast stain, (b, c) unsporulated and sporulated oocyst,
Figure 3.1. Isospora (a) modified acid-fast stain, (b, c) unsporulated and sporulated oocyst,