Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Geneticlab.ir
Urological Oncology
Mutations of RAS Gene Family in Specimens of
Bladder CancerNavaz Karimianpour,1 Parisa Mousavi-Shafaei,1 Abed-Ali Ziaee,1 Mohammad Taghi
Akbari,2 Gholamreza Pourmand,3 Amirreza Abedi,3 Ali Ahmadi,4 Hossein Afshin Alavi5
Introduction: Studies have shown different types of RAS mutations in
human bladder tumors with a wide range of mutation frequencies in different
patient populations. This study aimed to assess the frequency of specific-point
mutations in the RAS gene family of a group of Iranian patients with bladder
Methods: We examined the tumor specimens of 35 consecutive patients
with transitional cell carcinoma. The DNA samples were evaluated for the
occurrence of HRAS, KRAS, and NRAS activation using a polymerase chain
reaction-restriction fragment length polymorphism technique.
Results: None of the patients had mutations in the RAS gene family “hot
spots” including codons 12, 13, and 61.
Conclusion: We failed to find RAS mutations in our bladder tumor samples.
These observations may reflect the involvement of different etiological
factors in the induction of bladder tumor of which RAS mutation might not
molecular level, the RAS activating
of 3 functional genes, HarveyRAS(HRAS), Kristen RAS (KRAS), and
Mutation of RAS in Bladder Cancer—Karimianpour et al
Many studies have detected different types of
NRAS: 5’-GACATACTGGATACAGCTGGC-3’
RAS mutations in human bladder tumors.(8-14) The
results from these studies show a wide range of
mutation frequencies. It is not clear whether these
The DNA samples were amplified in a total
differences are related to the different life styles
volume of 50 μL of 10 × PCR buffer (5 μL),
of the studied populations, exposure to different
dNTP mix (10 mM, 1 μL), each primer (0.5 μL
suspected environmental carcinogens, or to the
with final concentration of 40 pmol each) and
sensitivity of ecogenetic relationships. According
Taq polymerase (Fermentas, Burlington, Canada).
to these observations, the present study was aimed
Amplification of fragments of the studied genes
to investigate the frequency of specific point
was carried out with a thermal cycler PCR (Geniu
mutations of the RAS gene family in a group of
system, Boehringer Mannheim, Germany) using
Iranian patients suffering from bladder cancer.
the following thermal profile: 95°C for 5 minutes,
32 cycles; HRAS: 95°C for 40 seconds, 6°C for 40
seconds, and 72°C for 45 seconds; KRAS: 94°C
for 40 seconds, 60°C for 40 seconds, and 72°C for
50 seconds; NRAS: 94°C for 30 seconds, 60°C for
Surgical specimens from 35 patients with
40 seconds, 72°C for 30 seconds, followed by a
histologically confirmed transitional cell
final extension at 72°C for 2 minutes.
carcinoma were collected and stored at -74°C.
The patients were consecutively selected from
among admitted patients to Sina Hospital. Age,
Restriction endonucleases MspI, BstNI, HphI,
sex, and smoking history of the patients were
and MscI (Fermentas, Burlington, Canada)
obtained from their hospital records.
digested codons 12 (HRAS), 12 and 13 (KRAS),
and 61 (NRAS), respectively. Any mutation at
these codons disrupts the restriction site for the
Genomic DNA was extracted from the tumoral
related restriction enzyme. Digestion was carried
tissues using proteinase K and phenol extraction
out in a total volume of 30 uL that contained 12
methods, and then, it was stored at 4°C.(15)
uL of PCR amplicon and 10 IU of restriction
endonuclease. Buffers and incubation conditions
(overnight at 37°C) were applied as recommended
by the manufactures. The digested fragments were
electrophoresed on a 6% polyacrylamide gel (1:59
Matched and mismatched oligonucleotide primers
bis-acrylamide for HRAS and KRAS genes, and
were designed or selected from previous studies
1:19 for NRAS gene) in 0.5 × TBE at 200 V for 1
for amplifying sequences around codon 12 of
hour and gels were stained in ethidium bromide.
HRAS, codons 12 and 13 of KRAS, and codon 61
In this work, different sizes of DNA fragments
of NRAS in order to generate subfragments only
of HRAS, NRAS,and KRAS genes (GenBank
from wild-type polymerase chain reaction (PCR)-
amplified RAS genes (mutant-type destroys the
and NM_004985, respectively) were obtained by
created restriction site).(16) The primer sequences
used were as follows: HRAS: 5’-GACGGAATATAAGCTGGTGG-3’
KRAS: 5’-ACTGAATATAAACTTGTGGTAG
The mean age of the patients was 65.8 ± 11.8
years (range, 34 to 85 years), and 74.3% of them
were older than 60 years. Twenty-nine patients
were men (82.8%) and 18 were smokers (51.4%).
Analysis of the pathological grades showed that
Mutation of RAS in Bladder Cancer—Karimianpour et al
23 specimens (65.7%) were low grade (2 low
malignant potential, 21 low grade, and 12 high
Polymerase Chain Reaction AmplificationThe lengths of the RAS amplified fragments
according to the designed primers were 420 bp,
65 bp, 144 bp for HRAS, NRAS, and KRAS genes,
Codon 12To determine any point mutation at codon 12
of HRAS, the restriction enzyme MspI was used.
Only the wild-type amplicon containing the
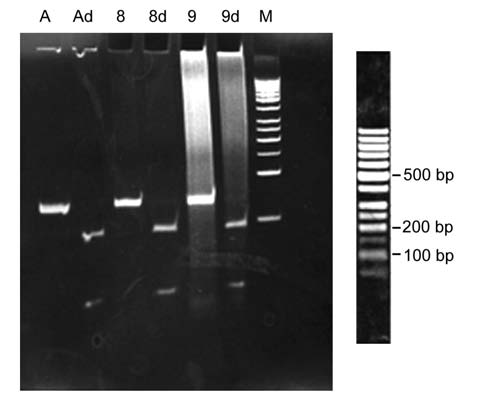
Figure 2.NRAS gene product analysis in bladder cancer
endonuclease recognition site could be cut off
by polymerase chain reaction-restriction fragment length
polymorphism. A, undigested DNA from a healthy person
and give rise to 390-bp and 30-bp fragments. No
(65-bp); Ad, MscI-cut polymerase chain reaction product of the
point mutation on codon 12 of HRAS was found
healthy person (44-bp and 21-bp); Lane 8 and 9, undigested
DNA of patients 8 and 9, respectively; and Lane 8d and 9d,
digested products of patients 8 and 9, respectively.
nucleotide change just before codon 61. In case of
any mutation, the restriction enzyme MscI would
be unable to cut the PCR fragment to 21-bp and
The restriction enzyme MscI was used for
digestion of the codon 61 of NRAS. The proper
cutting site (TGG↓CCA) was created with the
help of the forward primer, which led to a single
Codons 12 and 13The restriction enzyme BstNI was used for
codon 12 of KRAS gene digestion. A primer was
designed, so that the cutting site was created
just before codon 12. Only the wild-type
KRAS PCR product would be cut by BstN1,
yielding 2 fragments around 115-bp and 29-bp
oligonucleotides. For codon 13, GGTGA7/8↓ is
the recognition site for HphI and is cut off by the
enzyme. This site does not exist naturally, but it
would appear in any type of mutation. Digestion
reaction was carried out for each sample and no
mutation was detected for KRAS (Figure 3).
DISCUSSIONStudies on a variety of tumors have demonstrated
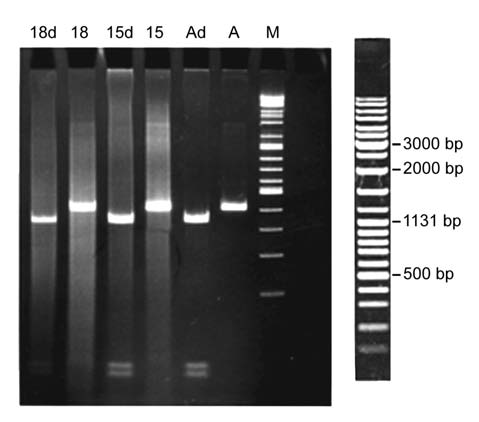
Figure 1.HRAS gene product analysis in bladder cancer
some “hot spots” in RAS gene family that are
by polymerase chain reaction-restriction fragment length
susceptible to point mutations. The frequent
polymorphism. A, undigested DNA from a healthy person
mutations are changes of glycine to valine at
(420-bp); Ad, MspI-cut polymerase chain reaction product
of the healthy person (390-bp and 30-bp); Lanes 15 and 18,
codon 12, glycine to cysteine at codon 13, and
undigested DNA of patients 15 and 18, respectively; and
glutamine to arginine/lysine/leucine at codon
Lane 15d and 18d, digested products of patients 15 and 18,
61.(17) The incidence of RAS mutation varies and is
Mutation of RAS in Bladder Cancer—Karimianpour et al
other hand, various levels of RAS mutation at
codon 12 have recently been reported in bladder
cancer. While Zhu and associates and Buyru and
coworkers showed 46.7% and 39% point mutation
of HRAS at codon 12, respectively,(3,12) Cattan and
associates detected only 1% of such alterations.(13)
Furthermore, Przybojewska and colleagues found
the HRAS mutation in 84% of patients with
bladder cancer using a PCR-restriction fragment
length polymorphism assay.(16) In contrast to the above discussed investigations
showing RAS activation, our study detected no
mutation in the RAS gene family in any grades of
bladder cancer in the 35 studied patients. It should
be mentioned that the RAS protein dysfunction
may occur not only as a result of mutations in the
RAS gene, but also due to changes in the protein
level. Quantitative alterations in the expression
Figure 3.KRAS gene product analysis in bladder cancer
due to gene amplification or overexpression could
by polymerase chain reaction-restriction fragment length
lead to continuous proliferative signals needed for
polymorphism. A, undigested DNA from a healthy person (144-bp);
cell propagation. Previous studies demonstrated
Ad, BstNI-cut polymerase chain reaction product of the healthy
person (115-bp and 29-bp); Lane 27, undigested DNA from patient
27; and Lane 27d, the digested product from patient 27.
carcinoma in situ and high-grade tumors, but
not in hyperplasia or low-grade tumors when
greatly dependent on the tissue or cell type from
immunohistochemical technique was applied.(14)
which the cancer cells are derived. Although RAS
Vageli and associates reported an increase in RAS
mutations occur in 75% to 95% of pancreatic
transcripts in about 40% of the bladder cancers,
carcinomas and 50% of colon carcinomas, they
as well.(25) All these studies indicate that the
are rare in several other neoplasms.(18-20) The
precise frequency of RAS mutations in human
HRAS mutation was first detected in the human
bladder cancer is still unclear. The observed
bladder cancer cell line T24.(7) Subsequent studies
discrepancies in the mutation pattern of RAS
demonstrated that HRAS mutations were more
gene family among different populations suffering
frequently observed in urinary tract tumors
from bladder cancer may either reflect different
than the KRAS or NRAS genes.(21) This initial
etiological mechanisms involved in disease
expectation has been materialized, since later
progression or alternative RAS dysfunction such
analysis of uncultured bladder tumors showed
as gene amplification and/or overexpression.(14,25)
that only about 10% of the samples contained
Notably, it is not surprising that Iranian patients
a mutated HRAS.(22-24) However, later reports
have a specific mutation pattern for P53 gene
showed higher frequencies. While Fitzgerald and
as it has been reported for esophageal cancer.(26)
associates reported mutations in the HRAS gene
Ecogenetic relationships and cultural conditions
in 44% of urine sediments from bladder cancer
of may somehow explain the absence of RAS gene
patients,(9) Czerniak and coworkers observed
family mutation in our patients. Although the
HRAS mutation specifically in connection to
results so far reported still remain controversial,
codon 12 in 45% of the bladder cancers.(10) Also,
activation of the RAS oncogene by point
in a recent study by Jebar and colleagues on 98
mutation or overexpression may be important
bladder tumors and 31 bladder cell lines, RAS
in the carcinogenesis and progression of human
mutation was detected in 13% of both types of
samples.(11) In total, there were 10 mutations
in HRAS, 4 in KRAS, and 4 in NRAS. On the
Smoking is an established risk factor for bladder
Mutation of RAS in Bladder Cancer—Karimianpour et al
cancer.(27) Consistent with the epidemiological
8. Oxford G, Theodorescu D. The role of Ras superfamily
evidence for an association between bladder
proteins in bladder cancer progression. J Urol.
cancer and smoking, we found that about 51% of
9. Fitzgerald JM, Ramchurren N, Rieger K, et al.
our patients were smokers, which shows a direct
Identification of H-ras mutations in urine sediments
correlation between smoking and the incidence
complements cytology in the detection of bladder
of bladder cancer. However, the group under
tumors. J Natl Cancer Inst. 1995;87:129-33.
our investigation is too small in number to be
10. Czerniak B, Cohen GL, Etkind P, et al. Concurrent
mutations of coding and regulatory sequences of
considered for epidemiological conclusions.
the Ha-ras gene in urinary bladder carcinomas. Hum
The other related risk factor of bladder cancer
is age. Our data showed nearly three-fourth of
11. Jebar AH, Hurst CD, Tomlinson DC, Johnston C,
our patients were over 60 years of age. This is in
Taylor CF, Knowles MA. FGFR3 and Ras gene
mutations are mutually exclusive genetic events in
accordance with the previous data showing more
urothelial cell carcinoma. Oncogene. 2005;24:5218-
than 65% of bladder cancer patients in the United
12. Zhu D, Xing D, Shen X, Liu J. A method to
quantitatively detect H-ras point mutation based on
electrochemiluminescence. Biochem Biophys Res
We failed to find RAS gene mutation in our
13. Cattan N, Saison-Behmoaras T, Mari B, et al.
patients with bladder tumors. This observation
Screening of human bladder carcinomas for the
presence of Ha-ras codon 12 mutation. Oncol Rep.
may reflect the involvement of different
etiological factors in the induction of this tumor.
14. Viola MV, Fromowitz F, Oravez S, Deb S, Schlom
Due to the reported studies and possibility of the
J. ras Oncogene p21 expression is increased
involvement of various etiological factors, it is
in premalignant lesions and high grade bladder
carcinoma. J Exp Med. 1985;161:1213-8.
interesting to study the situation among Iranian
patients suffering from bladder cancer with
15. Raply R. The nucleic acid protocols hand book.
Totowa, New Jersey: Human Press; 2000.
various pathological low-grade and high-grade
16. Przybojewska B, Jagiello A, Jalmuzna P. H-RAS,
tumors regarding the status of these three genes.
K-RAS, and N-RAS gene activation in human bladder
cancers. Cancer Genet Cytogenet. 2000;121:73-7.
17. Levesque P, Ramchurren N, Saini K, Joyce A,
Libertino J, Summerhayes IC. Screening of human
bladder tumors and urine sediments for the presence
of H-ras mutations. Int J Cancer. 1993;55:785-90.
18. Almoguera C, Shibata D, Forrester K, Martin J,
Arnheim N, Perucho M. Most human carcinomas of
1. Borden LS, Jr., Clark PE, Hall MC. Bladder cancer.
the exocrine pancreas contain mutant c-K-ras genes.
2. Jemal A, Murray T, Ward E, et al. Cancer statistics,
19. Smit VT, Boot AJ, Smits AM, Fleuren GJ, Cornelisse
2005. CA Cancer J Clin. 2005;55:10-30.
CJ, Bos JL. KRAS codon 12 mutations occur very
frequently in pancreatic adenocarcinomas. Nucleic
3. Buyru N, Tigli H, Ozcan F, Dalay N. Ras oncogene
mutations in urine sediments of patients with bladder
cancer. J Biochem Mol Biol. 2003;36:399-402.
20. Vogelstein B, Fearon ER, Hamilton SR, et al. Genetic
alterations during colorectal-tumor development. N
4. Bos JL. ras oncogenes in human cancer: a review.
21. Rabbani F, Cordon-Cardo C. Mutation of cell cycle
5. Varras MN, Koffa M, Koumantakis E, et al. ras gene
regulators and their impact on superficial bladder
mutations in human endometrial carcinoma. Oncology.
cancer. Urol Clin North Am. 2000;27:83-102, ix.
22. Fujita J, Srivastava SK, Kraus MH, Rhim JS, Tronick
6. Shinohara N, Koyanagi T. Ras signal transduction
SR, Aaronson SA. Frequency of molecular alterations
in carcinogenesis and progression of bladder
affecting ras protooncogenes in human urinary tract
cancer: molecular target for treatment? Urol Res.
tumors. Proc Natl Acad Sci U S A. 1985;82:3849-53.
23. Knowles MA, Williamson M. Mutation of H-ras is
7. Capon DJ, Chen EY, Levinson AD, Seeburg PH,
infrequent in bladder cancer: confirmation by single-
Goeddel DV. Complete nucleotide sequences of the
strand conformation polymorphism analysis, designed
T24 human bladder carcinoma oncogene and its
restriction fragment length polymorphisms, and direct
normal homologue. Nature. 1983;302:33-7.
sequencing. Cancer Res. 1993;53:133-9.
Mutation of RAS in Bladder Cancer—Karimianpour et al
24. Saito S, Hata M, Fukuyama R, et al. Screening of
of the esophagus in Iran. Oncogene. 2001;20:7368-
H-ras gene point mutations in 50 cases of bladder
carcinoma. Int J Urol. 1997;4:178-85.
27. Dolin PJ. An epidemiological review of tobacco use
25. Vageli D, Kiaris H, Delakas D, Anezinis P, Cranidis
and bladder cancer. J Smoking Rel Dis. 1991; 2 : 129-
A, Spandidos DA. Transcriptional activation of H-ras,
K-ras and N-ras proto-oncogenes in human bladder
tumors. Cancer Lett. 1996;107:241-7.
28. Jung I, Messing E. Molecular mechanisms and
pathways in bladder cancer development and
26. Sepehr A, Taniere P, Martel-Planche G, et al. Distinct
progression. Cancer Control. 2000;7:325-34.
pattern of TP53 mutations in squamous cell carcinoma
CLINICAL TRIAL REGISTRATIONThe Iranian Registry of Clinical Trials (IRCT) has been launched
(http://www.irct.ir/) thanks to the sponsorship by the Iranian Ministry of
Health. We strongly encourage researchers who would like to publish reports
of their clinical trial in Urology Journal to register their studies in the IRCT
or other registries that are proposed by the World Health Organization and
the International Committee of Medical Journal Editors. Registration of clinical trials before starting the research project is now
considered a primary requirement by these organizations, and it is also
emphasized by the World Medical Association Declaration of Helsinki. This
helps to ensure that decisions about healthcare are informed by all of the
available evidence, ensure that a trial and its results are publicly disclosed,
avoid unnecessary duplication, facilitate recruitment of participants, identify
gaps in research, encourage collaboration among researchers, and make it
possible to identify potential problems and improve clinical trials. The links below would help you to find clinical trial registries and useful
information on this issue:www.icmje.org/clin_trialup.htm
Pharma forum:Layout 1 25/02/2010 15:10 Page 1 Vista signs agreements with Quinn and Vhi V ista Primary Care, Ireland’s scans to its members. Commenting on the agreements, Mr uniquely capable of producing 4D vol-Quinn Healthcare members covered Ulick McEvaddy, Chairman of Vista, ume images.”campus for public and private by the arrangements with Vista Pri- said: ‘Since we opened our doo
SECONDA UNIVERSITÁ DEGLI STUDI DI NAPOLI FACOLTÁ DI MEDICINA E CHIRURGIA DIPARTIMENTO DI PSICHIATRIA, NEUROPSICHIATRIA INFANTILE, AUDIOFONIATRIA E DERMATOVENEREOLOGIA Direttore: Prof. Mario Maj IL DISTURBO POST-TRAUMATICO DA STRESS: VALUTAZIONE DELL’EFFICACIA DELL’EYE MOVEMENT DESENSITIZATION AND REPROCESSING IL DISTURBO POST- TRAUMATICO DA STRESS
 Mutation of RAS in Bladder Cancer—Karimianpour et al
23 specimens (65.7%) were low grade (2 low
malignant potential, 21 low grade, and 12 high
Polymerase Chain Reaction AmplificationThe lengths of the RAS amplified fragments
according to the designed primers were 420 bp,
65 bp, 144 bp for HRAS, NRAS, and KRAS genes,
Codon 12To determine any point mutation at codon 12
of HRAS, the restriction enzyme MspI was used.
Only the wild-type amplicon containing the
Figure 2. NRAS gene product analysis in bladder cancer
Mutation of RAS in Bladder Cancer—Karimianpour et al
23 specimens (65.7%) were low grade (2 low
malignant potential, 21 low grade, and 12 high
Polymerase Chain Reaction AmplificationThe lengths of the RAS amplified fragments
according to the designed primers were 420 bp,
65 bp, 144 bp for HRAS, NRAS, and KRAS genes,
Codon 12To determine any point mutation at codon 12
of HRAS, the restriction enzyme MspI was used.
Only the wild-type amplicon containing the
Figure 2. NRAS gene product analysis in bladder cancer 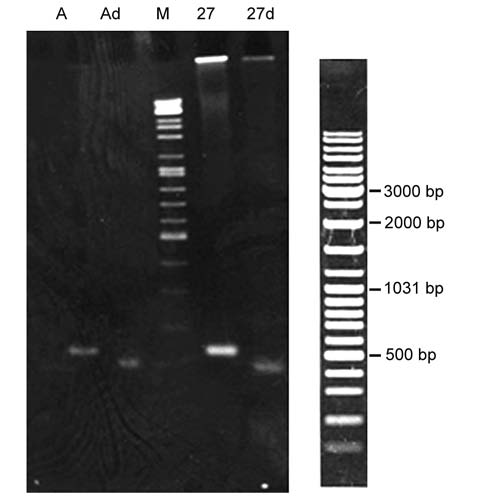 Mutation of RAS in Bladder Cancer—Karimianpour et al
other hand, various levels of RAS mutation at
codon 12 have recently been reported in bladder
cancer. While Zhu and associates and Buyru and
coworkers showed 46.7% and 39% point mutation
of HRAS at codon 12, respectively,(3,12) Cattan and
associates detected only 1% of such alterations.(13)
Furthermore, Przybojewska and colleagues found
the HRAS mutation in 84% of patients with
bladder cancer using a PCR-restriction fragment
length polymorphism assay.(16) In contrast to the above discussed investigations
showing RAS activation, our study detected no
mutation in the RAS gene family in any grades of
bladder cancer in the 35 studied patients. It should
be mentioned that the RAS protein dysfunction
may occur not only as a result of mutations in the
RAS gene, but also due to changes in the protein
level. Quantitative alterations in the expression
Figure 3. KRAS gene product analysis in bladder cancer
Mutation of RAS in Bladder Cancer—Karimianpour et al
other hand, various levels of RAS mutation at
codon 12 have recently been reported in bladder
cancer. While Zhu and associates and Buyru and
coworkers showed 46.7% and 39% point mutation
of HRAS at codon 12, respectively,(3,12) Cattan and
associates detected only 1% of such alterations.(13)
Furthermore, Przybojewska and colleagues found
the HRAS mutation in 84% of patients with
bladder cancer using a PCR-restriction fragment
length polymorphism assay.(16) In contrast to the above discussed investigations
showing RAS activation, our study detected no
mutation in the RAS gene family in any grades of
bladder cancer in the 35 studied patients. It should
be mentioned that the RAS protein dysfunction
may occur not only as a result of mutations in the
RAS gene, but also due to changes in the protein
level. Quantitative alterations in the expression
Figure 3. KRAS gene product analysis in bladder cancer