Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Untitled-
Management of Peripheral Arterial Disease DANIELA C. GEY, M.D., University of Heidelberg School of Medicine, Heidelberg, Germany EMIL P. LESHO, LTC, MC, USA, U.S. Army Medical Department Activity, Heidelberg, Germany JOHANNES MANNGOLD, M.D., Kreuzlingen Heart Center, Bodensee, Switzerland Peripheral arterial disease is common, but the diagnosis frequently is overlooked because of subtle physical findings and lack of classic symptoms. Screening based on the ankle brachial index using Doppler ultrasonography may be more useful than physical examination alone. Noninvasive modalities to locate lesions include magnetic resonance angiography, duplex scanning, and hemodynamic localization. Major risk factors for peripheral arterial disease are cigarette smoking, diabetes mellitus, older age (older than 40 years), hypertension, hyperlipidemia, and hyperhomocystinemia. Nonsurgical therapy for intermittent claudication involves risk-factor modification, exercise, and pharmaco- logic therapy. Based on available evidence, a supervised exercise program is the most effective treatment. All patients with peripheral arterial disease should undergo aggres- sive control of blood pressure, sugar intake, and lipid levels. All available strategies to help patients quit smoking, such as counseling and nicotine replacement, should be used. Effective drug therapies for peripheral arterial disease include aspirin (with or without dipyridamole), clopidogrel, cilostazol, and pentoxifylline. (Am Fam Physician 2004;69:525-32,533. Copyright 2004 American Academy of Family Physicians.)
may thwart effective secondary preven-tive strategies,2 including intensive treat-ment for hyperlipidemia, hypertension,
arterial disease (PAD) affects approximately 12 million persons in the
and smoking cessation. [Evidence level C,
study1 concluded that many physicians routinely do not obtain a relevant his-
Important Signs of Chronic Arterial Insufficiency
subtle signs of the condition on physi-cal examination (Tables 1 and 2). The underdiagnosis of PAD in primary care
Limb examination (and comparison with the opposite limb) includes:
Poor nail growth (brittle nails)Dry, scaly, atrophic skin
Differential Diagnosis of Intermittent Claudication
Pallor with leg elevation after one minute at
60 degrees (normal color should return in
Nonvascular causes
10 to 15 seconds; longer than 40 seconds
Ischemic tissue ulceration (punched-out,
pulses (especially after exercising the limb)
Vascular causes
Additional examination by palpation and aus-
Thromboangiitis obliterans (Buerger’s disease)
cultation to detect abnormal aortic aneurysm
See page 465 for defi-nitions of strength-of-evidence levels.
Downloaded from the American Family Physician Web site at www.aafp.org/afp. Copyright 2004 American Academy of Family Physicians. For the private, noncommercial
use of one individual user of the Web site. All other rights reserved. Contact copyrights@aafp.org for copyright questions and/or permission requests.
patients with PAD may not have the clas-sic symptoms of claudication.3 Some experts
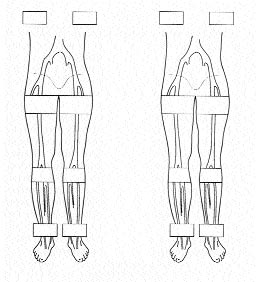
FIGURE 1. Dermatologic findings of peripheral
argue that a thorough physical examination
with special attention to the pulses, auscul-tation for arterial bruits, and inspection for
Diagnosis
postural color changes (Figure 1) can be almost as informative as an ABI using Dop-
Screening based on the ankle brachial index
Several factors complicate the diagnosis
phy could prove highly useful in identifying
patients with previously unrecognized PAD.2
proximal aneurysm or arterial occlusive dis-
In a recent multicenter study,3 the ABI corre-
ease distal to the ankle.4 Obtaining a medical
lated more closely with exercise capacity than
history also can be problematic.1,5 Although
did symptoms. This finding implies that many
83 percent of the patients in one large study2 knew they had PAD, only 49 percent of their physicians were aware of this history. More
than one half of patients identified as having PAD on the basis of an abnormal ABI value
do not have typical claudication symptoms, but they do have other types of leg pain on exertion, with reduced ambulatory activity and quality of life.3
dication or other symptoms if the occlusion develops slowly, allowing sufficient collateral
circulation to develop, or if the patient is mostly sedentary.4 Improving skills in eliciting symptoms, examining the peripheral vascular system, and obtaining segmental blood pres-sures (Figure 2),6 plus increased use of Doppler ABI in patients at risk of PAD, should identify
more patients in whom aggressive preventive strategies might delay disease progression or obviate the need for an invasive interven-tion.1,2
Treatment
dication involves risk-factor modification,
FIGURE 2. Segmental blood pressure measurement. A, segmental leg
exercise training, and pharmacologic therapy
pressures in a normal right extremity (ABI: 115/115 = 1.00) and one with
an isolated left iliac artery occlusion (ABI: 70/117 = 0.60). Horizontal and
vertical pressure gradients exist at the thigh. B, segmental leg pressures
RISK-FACTOR MODIFICATION
in a patient with an isolated focal right superficial femoral artery steno-
sis and a distal left tibial artery occlusion. (ABI = ankle brachial index)
hypertension, hyperlipidemia, age older than
Adapted with permission from Wilt TJ. Current strategies in the diagnosis and
40 years, and hyperhomocystinemia increase
management of lower extremity peripheral vascular disease. J Gen Intern Med 1992;7:91.
the risk of developing PAD. All patients with
PAD, regardless of the severity of symptoms,
should undergo risk-factor modification.
Currently, almost one fourth of adults in
Smoking. Smoking is the most important
the United States smoke cigarettes, and 70
risk factor and is correlated more closely
percent of smokers report that they want to
quit.9 Approximately one third of smokers
factor.7 Smoking cessation probably reduces
try to stop smoking each year, but only 20
the severity of claudication; however a meta-
percent seek professional help. Fewer than 10
analysis8 concluded that it did not improve
percent of smokers who attempt to quit on
maximal treadmill walking distance. [Evi-
their own are successful over the long term.9
dence level B, observational study] Cessation
Two approaches have strong evidence of effi-
of cigarette smoking reduces the progression
cacy for smoking cessation: pharmacotherapy
of disease, as shown by lower rates of amputa-
and counseling.9-11 Each is effective by itself,
tion and lower incidences of rest ischemia in
but the two combined achieve the highest
patients who quit, and it reduces the risks of
rates of smoking cessation.9,11 Clinical trials
myocardial infarction and death from other
have demonstrated that a physician’s advice
Management of Peripheral Arterial Disease
Assess for peripheral arterial disease.
profiles, hypertension, diabetes, hypercoagulability screen, homocysteine level, Lp(a) lipoprotein
(A1c <7.0 percent), smoking cessation (counseling and pharmacotherapy),
hypertension treatment (follow JNC-VI guidelines), LDL cholesterol <100 mg per dL (2.60 mmol per L), antiplatelet
scanning, hemodynamic localization, MRA, angiography.
FIGURE 3. Algorithm for the evaluation and management of patients with peripheral arte-
rial disease. (MWD = maximal walking distance; PFWD = pain-free walking distance; SF-36 =
medical outcomes short form 36 questionnaire; WIQ = walking impairment questionnaire; A1c
= hemoglobin A1c; JNC-VI = Sixth report of the Joint National Committee on Prevention, Detec-
tion, Evaluation, and Treatment of High Blood Pressure; LDL = low-density lipoprotein; MRA =
to stop smoking increases the rates of smok-
tight glycemic control decreases the incidence
ing cessation in patients by approximately
of intermittent claudication or critical limb
30 percent.12 Providing a brief three-min-
ischemia.13 However, minimizing hypergly-
ute counseling session is more effective than
cemia as a risk factor associated with the sub-
advising the patient to quit, and it doubles
sequent development of PAD could not only
the cessation rate compared with no interven-
decrease the rates of cardiovascular disease
tion.12 Too often, physicians miss this critical
and myocardial infarction, but also reduce the
comes (claudication, peripheral revascular-
(FDA) has approved six products for smok-
ization, or critical limb ischemia and ampu-
ing cessation: sustained-release bupropion
(Zyban) and five nicotine-replacement prod-
ucts (i.e., gum, lozenge, a transdermal patch,
Intensive insulin therapy elicited a trend
a nasal spray, and a vapor inhaler). The use
for reduced risk of important PAD outcomes
of all nicotine-replacement products increases
(claudication, peripheral revascularization, or
the long-term rates of smoking cessation and
amputation) by 22 percent. This result did
relieves cravings for nicotine and the symp-
not achieve statistical significance, because
toms of nicotine withdrawal. Nortriptyline
the study was not powered for assessment of
(Pamelor) and clonidine (Catapres) also have
this outcome. In other words, there is at least
been found to aid smoking cessation, but the
moderately strong, if statistically inconclusive,
FDA has not approved them for this indica-
evidence that macrovascular coronary (and
potentially limb) outcomes are improved with
Diabetes Mellitus. No controlled trials have
glycemic control, and these outcomes are
directly evaluated the effects of antidiabetic
central to good PAD care. Even in the absence
therapy on the natural history of PAD. Cur-
of high-quality clinical investigations, it is
rently, no prospective evidence shows that
important to note that diabetic control has an impact on limb infection and amputation in patients with severe PAD (critical limb
ischemia). Furthermore, because aggressive
DANIELA C. GEY, M.D., is a dermatology resident at the human immunodeficiency
control of blood glucose in type 1 and type
virus (HIV)/sexually transmitted disease clinic affiliated with the University of Heidel-
2 diabetes reduces the risk of microvascular
berg School of Medicine, where she received her medical degree. She is an investigator in two international, multicenter studies of immune augmentation with interleukin-2
complications, it also may benefit patients
in patients with HIV or acquired immunodeficiency syndrome, and has participated in
other research projects investigating experimental protease inhibitors. Hypertension. Hypertension is a major risk
EMIL P. LESHO, LTC, MC, USA, is currently an infectious diseases fellow at the National
factor for PAD, but the effect of antihyper-
Capital Consortium, Uniformed Services University of the Health Sciences, National
tensive therapy on the progression of disease
Naval Medical Center, Bethesda, Md., and Walter Reed Army Medical Center, Wash-ington, D.C. Dr. Lesho received his medical degree from Philadelphia College of
or the risk of claudication is unclear. Data
Osteopathic Medicine and completed an internal medicine residency at Madigan Army
derived from studies of cardiovascular disease
Medical Center, Tacoma, Wash. He was formerly with the Army Medical Department
support the aggressive treatment of hyperten-
sion in patients with PAD.7 Although no data
JOHANNES MANNGOLD, M.D., is a first-year resident in internal medicine at the Kreuz-
demonstrate an impact of antihypertensive
lingen Heart Center, Bodensee, Switzerland. He completed his undergraduate and medical school training at the University of Heidelberg School of Medicine, Heidelberg,
therapy on PAD outcomes, this lack of data is
because PAD-related event rates are low. The
Address correspondence to Emil P. Lesho, LTC, MC, USA, 611 Forest Glen Rd., Silver
power to detect such outcomes would require
Spring, MD 20901 (e-mail: emillesho@yahoo.com). Reprints are not available from
a trial larger than the recent Antihypertensive
and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) effort, and a
trial of efficacy would ethically require an active comparator intervention, making the
Exercise training is the most effective treatment of peripheral
assessment of PAD-specific and drug-specific
Hypertension should be controlled in these
patients primarily to reduce morbidity from cardiovascular and cerebrovascular disease.
min B12 metabolism, and dietary folate defi-
The use of beta blockers in patients with inter-
ciency. Although supplementing the diet with
mittent claudication was of concern because
B vitamins and folate usually lowers serum
several early case reports documented wors-
homocysteine concentrations,27 no controlled
ening claudication and decreasing blood flow
trials demonstrate that reducing serum homo-
in the legs of patients taking these drugs. A
cysteine concentration is beneficial in patients
later meta-analysis and critical review con-
with PAD.28 PAD is not a contraindication to
cluded that beta-adrenergic antagonists are
estrogen therapy, but estrogen should not be
safe in patients with PAD, except in those
recommended for treating PAD in postmeno-
most severely affected. Even in these patients,
the drugs can be administered, but with cau-tion.15,16
Hyperlipidemia. Several large clinical tri-
Exercise. A formal exercise program is
als have demonstrated the benefits of lipid-
the most effective treatment of PAD, and
lowering therapy in patients with PAD who
effectiveness was demonstrated in more than
have coexisting coronary and cerebral arterial
20 controlled trials.30-33 Exercise increased
disease.17-25 Simvastatin (Zocor) drastically
the distance to onset of claudication by 179
lowered cardiovascular ischemic event rates
percent in a meta-analysis of 21 published
in the large PAD subgroup, despite initial low
studies.33 The greatest improvements in walk-
low-density lipoprotein (LDL) levels.25 Lipid
ing ability occur when each exercise session
normalization has been shown to reduce dis-
lasts longer than 30 minutes, when sessions
ease progression and the severity of claudica-
take place at least three times per week, when
tion.17-25 The current recommendation for
the patient walks until near-maximal pain
patients is to achieve a serum LDL cholesterol
is reached in each session, and when the
concentration of less than 100 mg per dL
program lasts at least six months.33 These
(2.6 mmol per L) and a serum triglyceride
improvements were sustained when patients
concentration of less than 150 mg per dL
continued to participate in a maintenance
(3.9 mmol per L).18 A statin drug should be
given as initial therapy, but niacin also is a
Another meta-analysis34 from the Cochrane
consideration because it increases serum high-
Collaboration that considered only random-
density lipoprotein (HDL) concentrations and
ized controlled trials showed that exercise
lowers serum triglyceride concentrations with-
produced significant improvements in walk-
out (as formerly believed) worsening glucose
antiplatelet therapy. Motivated patients in
Hyperhomocystinemia. A high serum homo-
a supervised setting modeled after cardiac
cysteine concentration is an independent risk
rehabilitation had the best results.33 The large,
factor for PAD and is associated with an
exercise-induced improvements in function
increased risk of death from cardiovascular
and symptoms that occur in patients with
causes.26 The causes of high serum homocys-
claudication do not appear to be caused by
teine concentrations include genetic defects in
an increased collateral blood flow but by
homocysteine metabolism, alterations in vita-
other mechanisms.33 Such potential mecha-
TABLE 3 Pharmacotherapy for Patients with Claudication
Recommended by the American College of Chest
Physicians for PAD, but the FDA found insufficient
evidence to approve labeling for this indication
Fewer side effects than aspirin in the CAPRIE trial;
significantly less risk for TTP than ticlopidine
May have a small effect on walking ability, but
insufficient data to support widespread use
Correct dosing is critical; avoid in patients with heart
failure; reduce dosing to 50 mg twice per day in
patients taking calcium channel blockers; may
500 mg per day orally Extensive hemodynamic monitoring for risk of TTP
600 mg per day orally Serotonin antagonist; increased walking distance
in several trials, but use remains controversial;
iloprost, prostaglandin E1 orally, or 60 mcg [Alprostadil])
Promising results in uncontrolled trials
Effective, but study methodology questionable
PAD = peripheral arterial disease; FDA = U.S. Food and Drug Administration; CAPRIE = Clopidogrel versus Aspirin in Patients at Risk of Ischemic Events; TTP = thrombotic thrombocytopenic purpura.
nisms include improvements in endothelial
reactions and because of the availability of
vasodilator function, inflammatory responses,
newer safer agents (Table 3). Aspirin and
skeletal-muscle metabolism, enhanced oxy-
dipyridamole (Persantine) increase the pain-
gen availability by improved blood viscosity,
free walking distance and resting limb blood
and lessened ischemia at any achieved work-
flow, or lead to an improved coagulation
The recent publication of a current proce-
In the Clopidogrel versus Aspirin in Patients
dural terminology (CPT) code for PAD exer-
at Risk of Ischemic Events (CAPRIE) trial,36
cise reflects the importance of exercise therapy
75 mg of clopidogrel was slightly but sig-
nificantly better than 325 mg of aspirin in
Terminology, American Medical Association,
the total population for preventing strokes,
myocardial infarction, and vascular disease.36
Pharmacologic Therapy. Although a meta-
The PAD subgroup with nearly 6,500 patients
analysis of randomized studies of antiplatelet
agents found that ticlopidine (Ticlid) had
spective PAD clinical trial and demonstrated
the best evidence of efficacy in improvement
a profound superiority in the PAD popula-
in walking distance and reduction in occlu-
tion treated with clopidogrel compared with
sion,7,28 it is no longer used because it has been
aspirin alone.36 This result led to the FDA
associated with life-threatening hematologic
approval of clopidogrel (Plavix) for the sec-
ondary prevention of atherosclerotic events in patients with PAD. National guidelines currently recommend aspirin (with or
Pentoxifylline (Trental), a rheologic modi-
without dipyridamole) or clopidogrel as first-choice drugs for
fier that also has an antiplatelet effect, was
approved in 1984 for the treatment of clau-dication. Pentoxifylline is less effective than cilostazol (Pletal).28,35 Two meta-analyses and two systematic reviews of pentoxifylline con-
in Europe, macrolide antibiotic treatment for
cluded that although the drug may have a
chlamydia infection, propionyl levocarnitine,
small effect on walking ability, the data are
defibrotide, ginkgo biloba, hyperbaric oxy-
insufficient to support its widespread use.28,35
gen, and angiogenic growth factors. Of these,
In a more recent controlled trial,36 pent-
angiogenic growth factors are perhaps the
oxifylline was significantly superior to placebo
most promising.35 For an in-depth, evidence-
in improving walking distance after six and
based review of PAD management, physicians
may refer to the Trans Atlantic Inter-Society
Cilostazol inhibits phosphodiesterase 3, sup-
presses platelet aggregation, activates lipopro-tein lipase, and causes arterial dilation.7,28,35
The authors indicate that they do not have conflicts
Approved in 1999 by the FDA for the treat-
of interest. Sources of funding: none reported.
ment of claudication, it improved pain-free
The opinions and assertions contained herein are
and maximal treadmill walking distance in
the private views of the authors and are not to be
randomized controlled trials compared with
construed as official or as reflecting the views of the
placebo or pentoxifylline.7,28,35 Correct dos-
U.S. Army Medical Department or the U.S. Army
ing is important, because 100 mg orally twice
per day significantly improved claudication
symptoms, while 100 mg per day did not.38 Cilostazol should not be used in patients
1. Ouriel K. Detection of peripheral arterial disease in
with heart failure.7,28 The dosage should be
2. Hirsch AT, Criqui MH, Treat-Jacobson D, Regen-
reduced to 50 mg orally twice per day when
steiner JG, Creager MA, Olin JW, et al. Peripheral
arterial disease detection, awareness, and treat-ment in primary care. JAMA 2001;286:1317-24.
because serum drug levels are elevated in these
3. McDermott MM, Greenland P, Liu K, Guralnik JM,
patients. Common side effects of cilostazol
Celic L, Criqui MH, et al. The ankle brachial index
include loose stool and gastric upset.7,28,35
is associated with leg function and physical activity: the Walking and Leg Circulation Study. Ann Intern
In summary, aspirin generally is considered
the antiplatelet drug of first choice. The 6th
4. Gaylis H. Diagnosis and treatment of peripheral
arterial disease. JAMA 2002;287:313.
5. Merenstein JH. Diagnosis and treatment of periph-
that aspirin alone (81 to 325 mg per day) or
eral arterial disease. JAMA 2002;287:314.
in combination with dipyridamole, should be
6. Wilt TJ. Current strategies in the diagnosis and
given indefinitely because it can modify the
management of lower extremity peripheral vascu-lar disease. J Gen Intern Med 1992;7:87-101.
natural history of intermittent claudication
7. Regensteiner JG, Hiatt WR. Current medical thera-
and those with high risk for future cardiovas-
pies for patients with peripheral arterial disease: a
cular events.39 These guidelines also suggest
critical review. Am J Med 2002;112:49-57.
8. Girolami B, Bernardi E, Prins MH, Ten Cate JW,
that clopidogrel may be superior to aspirin
Hettiarachchi R, Prandoni P, et al. Treatment of
and should be considered as an alternative
intermittent claudication with physical training,
treatment in these patients.39 Experimental
smoking cessation, pentoxifylline, or nafronyl: a meta- analysis. Arch Intern Med 1999;159:337-
or investigational agents for PAD include
naftidrofuryl (Nafronyl), which is approved
9. Rigotti NA. Clinical practice. Treatment of tobacco
use and dependence. N Engl J Med 2002;346:506-
trol of the Hyperlipidemias (POSCH). N Engl J Med
10. A clinical practice guideline for treating tobacco
24. Pedersen TR, Kjekshus J, Pyorala K, Olsson AG,
use and dependence: a U.S. Public Health Service
Cook TJ, Muslinger TA, et al. Effect of simvastatin
on ischemic signs and symptoms in the Scandina-
11. Krupski WC, Nguyen HT, Jones DN, Wallace H,
vian simvastatin survival study (4S). Am J Cardiol
Whitehill TA, Nehler MR. Smoking cessation coun-
seling: a missed opportunity for general surgery
25. Heart Protection Study Collaborative Group. MRC/
trainees. J Vasc Surg 2002;36:257-62.
BHF Heart Protection Study of cholesterol lower-
12. Fiore M. Treating tobacco use and dependence.
ing with simvastatin in 20,536 high-risk individu-
Rockville, Md.: U.S. Dept. of Health and Human
als: a randomised placebo-controlled trial. Lancet
Services, Public Health Service, 2000. (Also avail-
able at http://www.surgeongeneral.gov/tobacco).
26. Graham IM, Daly LE, Refsum HM, Robinson K,
13. Beckman JA, Creager MA, Libby P. Diabetes and
Brattstrom LE, Ueland PM, et al. Plasma homocys-
atherosclerosis: epidemiology, pathophysiology,
teine as a risk factor for vascular disease. JAMA
and management. JAMA 2002;287:2570-81.
14. Adler AI, Stevens RJ, Neil A, Stratton IM, Boulton
27. Jacques PF, Selhub J, Bostom AG, Wilson PW,
AJ, Holman RR. UKPDS 59: hyperglycemia and
Rosenberg IH. The effect of folic acid fortification
other potentially modifiable risk factors for periph-
on plasma folate and total homocysteine concen-
eral vascular disease in type 2 diabetes. Diabetes
trations. N Engl J Med 1999;340:1449-54.
28. Hiatt WR. Medical treatment of peripheral arterial
15. Radack K, Deck C. Beta-adrenergic blocker therapy
disease and claudication. N Engl J Med 2001;344:
does not worsen intermittent claudication in sub-
jects with peripheral arterial disease. A meta-analy-
29. Hulley S, Furberg C, Barrett-Connor E, Cauley J,
sis of randomized controlled trials. Arch Intern Med
Grady D, Haskell W, et al. Noncardiovascular dis-
ease outcomes during 6.8 years of hormone ther-
16. Solomon SA, Ramsay LE, Yeo WW, Parnel L, Morris-
apy: Heart and Estrogen/progestin Replacement
Jones W. Beta blockade and intermittent claudica-
Study follow-up (HERS II). JAMA 2002;288:58-66.
tion: placebo control ed trial of atenolol and nifedip-
30. Ohta T, Sugimoto I, Takeuchi N, Hosaka M, Ishi-
ine and their combination. BMJ 1991;303:1100-4.
bashi H. Indications for and limitations of exercise
17. LaRosa JC, He J, Vupputuri S. Effect of statins on
training in patients with intermittent claudication.
risk of coronary disease: a meta-analysis of ran-
domized controlled trials. JAMA 1999;282:2340-
31. Gardner AW, Katzel LI, Sorkin JD, Goldberg AP.
Effects of long-term exercise rehabilitation on
18. Ansell BJ, Watson KE, Fogelman AM. An evidence-
claudication distances in patients with peripheral
based assessment of NCEP Adult Treatment Panel
arterial disease: a randomized controlled trial. J
II guidelines. JAMA 1999;282:2051-7.
19. Elam MB, Hunninghake DB, Davis KB, Garg R, John-
32. Langbein WE, Collins EG, Orebaugh C, Maloney
son C, Egan D, et al. Effect of niacin on lipid and lipo-
C, Williams KJ, Littooy FN, et al. Increasing exercise
protein levels and glycemic control in patients with
tolerance of persons limited by claudication pain
diabetes and peripheral arterial disease: the ADMIT
using polestriding. J Vasc Surg 2002;35: 887-93.
study: a randomized trial. JAMA 2000;284:1263-
33. Stewart KJ, Hiatt WR, Regensteiner JG, Hirsch AT.
Exercise training for claudication. N Engl J Med
20. Blankenhorn DH, Azen SP, Crawford DW, Nessim SA,
Sanmarco ME, Selzer RH, et al. Effects of colestipol-
34. Leng GC, Fowler B, Ernst E. Exercise for intermit-
niacin therapy on human femoral atherosclerosis.
tent claudication. Cochrane Database Syst Rev
21. Buchwald H, Bourdages HR, Campos CT, Nguyen P,
35. Ouriel K. Peripheral arterial disease. Lancet 2001;
Williams SE, Boen JR. Impact of cholesterol reduc-
tion on peripheral arterial disease in the Program
36. A randomised, blinded, trial of clopidogrel versus
on the Surgical Control of the Hyperlipidemias
aspirin in patients at risk of ischaemic events
(CAPRIE). CAPRIE Steering Committee. Lancet
22. Duffield RG, Lewis B, Miller NE, Jamieson CW,
Brunt JN, Colchester AC. Treatment of hyperlipi-
37. De Sanctis MT, Cesarone MR, Belcaro G, Nicolaides
daemia retards progression of symptomatic femo-
AN, Griffin M, Incandela L, et al. Treatment of
ral atherosclerosis. A randomised controlled trial.
long-distance intermittent claudication with pent-
oxifylline: a 12-month, randomized trial. Angiology
23. Buchwald H, Varco RL, Matts JP, Long JM, Fitch LL,
Campbell GS, et al. Effect of partial ileal bypass
38. Strandness DE Jr, Dalman RL, Panian S, Rendell
surgery on mortality and morbidity from coronary
MS, Comp PC, Zhang P, et al. Effect of cilostazol in
heart disease in patients with hypercholesterol-
patients with intermittent claudication: a random-
emia. Report of the Program on the Surgical Con-
ized, double-blind, placebo-controlled study. Vasc
Basic Requirements Propecia—can donate 4 weeks after last doseBe 17 years of age—there is no upper limitProscar—can donate 4 weeks after last doseSoriatane (Acitretin)—can donate 3 years after last doseApheresis donation may have additional requirementsThyroid medication—can donate if stabilized Donation Frequency Medical conditions Platelet donors may donate every 48 hours
 Management of Peripheral Arterial Disease
Management of Peripheral Arterial Disease
 patients with PAD may not have the clas-sic symptoms of claudication.3 Some experts
FIGURE 1. Dermatologic findings of peripheral
argue that a thorough physical examination
with special attention to the pulses, auscul-tation for arterial bruits, and inspection for
Diagnosis
patients with PAD may not have the clas-sic symptoms of claudication.3 Some experts
FIGURE 1. Dermatologic findings of peripheral
argue that a thorough physical examination
with special attention to the pulses, auscul-tation for arterial bruits, and inspection for
Diagnosis