Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Microsoft word - msd_4457580123803433
Effects of childhood body size on breast cancer tumour characteristics
Jingmei Li1,2, Keith Humphreys1, Louise Eriksson1, Kamila Czene1, Jianjun Liu2 and Per
1Karolinska Institutet, Department of Medical Epidemiology and Biostatistics, Box 281, 171
2Human Genetics, Genome Institute of Singapore, 60 Biopolis Street, Singapore, 138672,
Corresponding author: Jingmei Li, Jingmei.Li@ki.se Abstract Introduction:Although a role of childhood body size in postmenopausal breast cancer risk
has been established, less is known about its influence on tumour characteristics.
Methods:We studied the relationships between childhood body size and tumour
characteristics in a Swedish population-based case-control study consisting of 2,818 breast
cancer cases and 3,111 controls. Our classification of childhood body size was derived from a
nine-level somatotype. Relative risks were estimated by odds ratios with 95% confidence
intervals, derived from fitting unconditional logistic regression models. Association between
somatotype at age 7 and tumour characteristics were evaluated in a case-only analysis where
P-values for heterogeneity were obtained by performing one degree of freedom trend tests.
Results: A large somatotype at age 7 was found to be associated with decreased
postmenopausal breast cancer risk. Although strongly associated with other risk factors such
as age of menarche, adult body mass index and mammographic density, somatotype at age 7
remained a significant protective factor (odds ratio (OR) comparing large to lean somatotype
at age 7 = 0.73, 95% confidence interval (CI) = 0.58-0.91, P trend = 0.004) after adjustment.
The significant protective effect was observed within all subgroups defined by estrogen
receptor (ER) and progesterone receptor (PR) status, with a stronger effect for ER-negative
(0.40, 95% CI = 0.21-0.75, P trend = 0.002), than for ER-positive (0.80, 95% CI = 0.62-1.05,
P trend = 0.062), tumours (P heterogeneity = 0.046). Somatotype at age 7 was not associated
with tumour size, histology, grade or the presence or absence of metastatic nodes.
Conclusions: Greater body size at age 7 is associated with a decreased risk of
postmenopausal breast cancer, and the associated protective effect is stronger for the ER-
negative breast cancer subtype than for the ER-positive subtype.
2010 Li et al.; licensee BioMed Central Ltd. This is an open access article distributed under
the terms of the Creative Commons Attribution License
(http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and
reproduction in any medium, provided the original work is properly cited.
Introduction {1st Level Heading}
There is considerable evidence that childhood anthropometric measurements are associated
with postmenopausal breast cancer risk. It has been consistently shown that variables that
approximate body shape and size early in life are inversely associated with breast cancer risk
in adulthood. For example, a study conducted in 1998 on the same data set as used in the
current study [1] reported that a larger somatotype at age seven years was associated with a
lower postmenopausal breast cancer risk. Likewise, Hilakivi-Clarke and colleagues [2] found
that a shorter height and higher body mass in girls from age 7 to 15 years were associated
with a decreased incidence of breast cancer. Berkey and colleagues [3] also found extremely
lean body mass at age 10 years to be associated with elevated breast cancer risk. In another
study performed in 141,393 Danish girls, a high childhood body mass index (BMI) at age 14
years was shown to be protective against breast cancer later on in life [4]. In addition, a study
performed on the large Nurses’ Health Study dataset concluded that average body fatness
between the ages of 5 and 10 years are inversely associated with mammographic density [5],
which is generally considered to be an intermediate phenotype of breast cancer [6].
Although a role of childhood body size in adult breast cancer risk has been established, less is
known about its influence on tumour characteristics. One study by Bardia and colleagues [7]
looked into the risk of developing postmenopausal breast cancer stratified by estrogen
receptor (ER) and progesterone receptor (PR) subtypes and reported that an increase in weight
at age 12 years was associated with a decrease in adult breast cancer risk, with the most
pronounced effects exhibited by ER-positive/PR-negative tumours. No significant
heterogeneity, however, was observed between the tumour subtypes studied. To our
knowledge, no other study has been conducted to assess whether pre-/peri-pubertal
measurements of body size can also influence tumour characteristics. We thus followed up on
the work of Bardia and colleagues and in the present study examined the relations between
childhood body size to address if the far-reaching effects of childhood body size have any
influence on tumour characteristics in adult cancers.
Materials and methods {1st Level Heading} Subjects {2nd Level Heading}
The subjects included in the current study are drawn from a population-based case-control
study of postmenopausal breast cancer in Swedish-born women aged 50 to 74 years at the
time of enrolment, which was between 1 October, 1993 and 31 March, 1995. Controls were
randomly selected from the Swedish registry and frequency matched to the expected age
distribution of the cases. Details on data collection and subjects have been described
previously [1]. The final study group included 2,818 cases and 3,111 controls. Approval of
the study was given by the ethical review board at the Karolinska Institutet (Stockholm,
Sweden) and six other ethical review boards in the respective regions from which the subjects
Data collection and classification {2nd Level Heading}
With the exception of clinical data on tumour characteristics and mammographic density, all
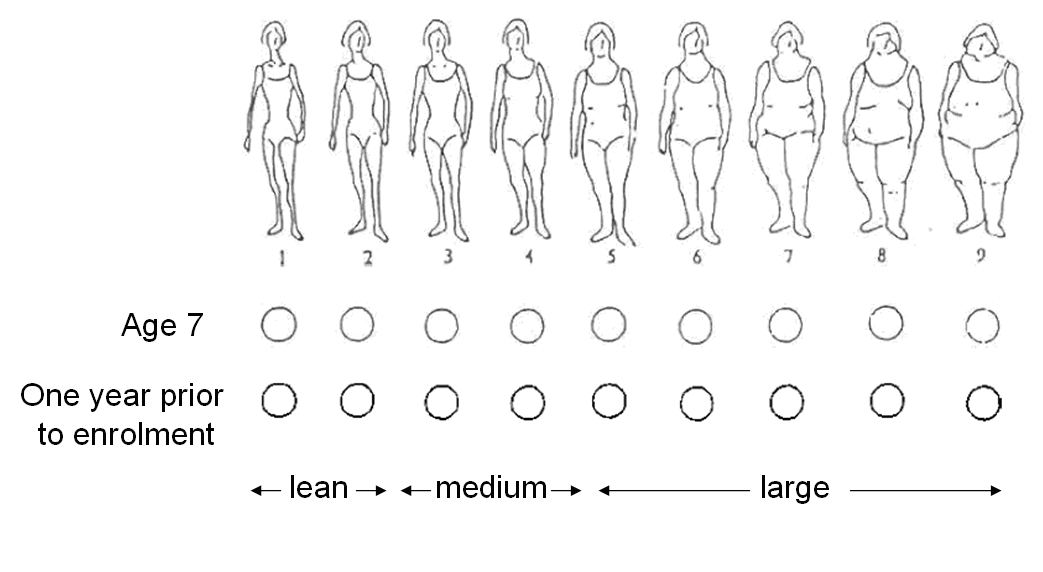
other covariate data were derived from the parent case-control study. Anthropometric
measurements at age seven years and one year prior to enrolment were collected by means of
a nine-level somatotype (Figure 1) featured in the study questionnaire, and the validity of this
measurement method has been previously described [1]. These pictograms have been
validated against BMI within a cohort of 100 Caucasian women from middle-class
communities with an average age of 73.1 years [8]. In a population-based validation study,
111 Swedish women aged 51 to 66 years were found to have a correlation coefficient between
BMI from school records and adult report of somatotype at age seven years of 0.6 [1]. The
somatotypes were subsequently grouped as lean (S1 to S2), medium (S3 to S4) and large (S5
to S9) prior to analysis. Other covariate data that was collected using the self-reported study
questionnaire and examined in this study include age of menarche (continuous, in years),
parity (continuous, number of live births), history of benign breast disease (binary,
never/ever), BMI (continuous, in kg/m2), history of hormone replacement therapy (HRT)
(binary, never/ever), and family history of breast cancer (binary, no/yes). Age at menopause
(continuous, in years) was also derived from information collected in the study questionnaire
and the definition used in this study has been previously described [1]. It is defined as the age
at the last menstrual period or the age at bilateral oophorectomy, if one year or more prior to
data collection. Women who have had a hysterectomy, or who have not ceased menstruation
due to HRT, or with missing information on age at menopause were considered to be
postmenopausal if the age reported at time of questionnaire was equal to or above the 90th
percentile of age at natural menopause of study subjects (current smokers: 54 years old;
nonsmokers: 55 years old, independent of case/control status). Subjects classified as
postmenopausal in this manner were assigned an age at menopause according to their current
smoking status and the mean ages at natural menopause in our data. Otherwise, women were
considered to be premenopausal and were excluded.
Information regarding the retrieval of tumour characteristics from the medical records of all
participants from surgical and oncological units throughout Sweden have been presented in
detail elsewhere [9, 10]. The tumour characteristics in the present study included tumour size
(categorical, groups in cm), grade (categorical, classified according to the Nottingham
histological grade or Bloom-Richardson scale), as well as ER and PR status (binary,
The process of collecting mammographic density data in this study has been described
previously [11]. Film mammograms of the medio-lateral oblique view were digitised using an
Array 2905HD Laser Film Digitizer (Array Corporation, Tokyo, Japan), which covers a range
of 0 to 4.7 optical density. For controls, breast side was randomized. For cases, the side
contralateral to the tumour was used. The density resolution was set at 12-bit spatial
resolution. The Cumulus software used for the computer-assisted thresholding was developed
at the University of Toronto [12]. For each image, a trained observer (LE) set the appropriate
gray-scale threshold levels defining the edge of the breast and distinguishing dense from non-
dense tissue. The software calculated the total number of pixels within the entire region of
interest and within the region identified as dense. These values were used to calculate the
percentage of the breast area that is dense. A random 10% of the images were included as
replicates to assess the intra-observer reliability, which was high with a Spearman rank
correlation coefficient of 0.95. However, as not all women attended mammographic
screenings, and some mammograms were missing, such information was available for only a
subset of the subjects (n = 3232, 54.5%).
Statistical analyses {2nd Level Heading}
The distribution of baseline characteristics of known breast cancer risk factors were
summarised as means and standard deviations or proportions. Odds ratio (OR) estimates with
corresponding 95% confidence intervals (CI) were computed by fitting unconditional logistic
regression models with breast cancer risk status as the response variable, adjusting for age.
To identify potential confounders of the association between somatotype at age seven years
and breast cancer risk, linear/logistic regression models were fitted for either continuous (age
of menarche, age of menopause, parity, BMI, and mammographic density) or binary (benign
breast disease and HRT) outcomes including only controls in the analysis. Somatotype at age
seven years was treated as a categorical (three-level) independent variable. Proportional odds
logistic regression was used in situations where the outcome variable was ordinal
(somatotypes at age seven years and one year prior to enrolment) from which cumulative OR
esimates with corresponding 95% CIs were computed. Covariates were considered potential
confounders if there was a priori evidence in the published literature of the factor being
associated with both childhood body size and breast cancer risk, or if the factor was
significantly associated at the 5% level with both somatotype at age seven years and breast
cancer risk. Those covariates that, when added to the model, changed the coefficient by more
than 10%, were considered confounders and adjusted for in the multivariate analysis. The
final variables in the multivariate logistic regression model examining breast cancer risk
overall, and stratified by ER and PR tumour subtypes, included age, age at menarche, benign
breast disease, and BMI one year prior to enrolment (recent BMI). Adjustment for other
variables did not influence the somatotype risk estimates. Mammographic density was also
identified as a confounder. However, as mammographic density data are only available for a
subset of the subjects, this variable was accounted for together with the other risk factors in a
separate model. Women with and without mammographic density information were not found
to differ significantly at the 5% level for the covariates included in the analysis models (data
Associations between somatotype at age seven years and tumour characteristics were
evaluated in a case-only analysis, by fitting ordinal regression models treating tumour
characteristics as dependent variables, with somatotype at age seven years included as a
covariate. P values for heterogeneity were obtained by performing one degree of freedom
trend tests. As there exists prior evidence that certain tumour characteristics such as ER status
are associated with age at diagnosis [13], and that somatotype at age seven years is
significantly associated with age of diagnosis at the 5% level (regression coefficient for age in
years of -0.91with corresponding 95% CI of -1.32 to -0.50), every model fitted in the case-
only analysis was also adjusted for age at diagnosis. All analyses were performed using the
statistical software R for Windows version 2.8.0 (R Development Core Team, Vienna,
Austria) [14]. The level of significance was set at 5%. All statistical tests were two-sided.
Results {1st Level Heading}
Table S1 in Additional file 1 describes the characteristics of study subjects with respect to
several breast cancer risk factors. Age of menarche was weakly but positively associated with
the disease (OR per year increase in age of menarche = 0.96, 95% CI = 0.93 to 1.00, P =
0.057), a result consistent with the literature [4]. Family history, age at menopause, parity, age
of first birth, benign breast disease, mammographic density, recent BMI and use of HRT were
strongly significant for breast cancer risk with effects in a direction consistent with those
estimated in other epidemiological studies. The first association analyses we performed
between somatotypes at different ages and breast cancer risk were adjusted for age at
enrolment only. Among the different measurements of somatotypes, only the time point at age
seven years was found to affect breast cancer risk (OR per increase in somatotype class =
0.87, 95% CI = 0.8 to 0.95, P = 0.001). A larger proportion of cases than controls had a leaner
body shape at age seven years. Despite somatotype one year prior to enrolment having a high
correlation to recent BMI (Spearman correlation coefficient: 0.760, data not shown), it was
not found to be significantly associated with breast cancer (OR per increase in somatotype
class = 1.04, 95% CI = 0.94 tp 1.15, P = 0.160).
To identify potential confounders of the association between somatotype at age seven years
and breast cancer risk, we assessed whether other established risk factors for breast cancer are
associated with somatotype at age seven years. An increase in childhood body size was found
to exhibit strong inverse associations with age of menarche (OR comparing large to lean
somatotype at age seven years = 0.61, 95% CI = 0.50 to 0.76, P trend<0.0001), benign breast
disease (0.47, 95% CI = 0.25 to 0.89, P trend = 0.006), and mammographic density (0.61,
95% CI = 0.41 to 0.90, P trend = 0.001; Table 1). Associations in the opposite direction were
found for proxy measures of physique at other time points, such as birth weight (OR
comparing birthweight >4000g to ≤2500g = 1.89, 95% CI = 0.95 to 3.76, P trend = 0.014),
somatotype one year prior to enrolment (OR comparing large to lean somatotype at age seven
years = 2.33, 95% CI = 1.70 to 3.18, P trend<0.0001) and recent BMI (2.66, 95% CI = 1.47 to
4.83, P trend<0.0001). No evidence of association was found between age of menopause and
somatotype at age seven years or between family history and somatotype at age seven years.
Parity and HRT were found to be independent of somatotype at age seven years (0.93, 95%
CI = 0.76 to 1.13, P trend = 0.217 and 0.98, 95% CI = 0.73 to 1.32, P trend = 0.868,
After adjustment of known breast cancer predictors and other associated risk factors, the
inverse association of somatotype at age seven years with breast cancer remained highly
significant (Table 2; OR comparing large to lean somatotype at age seven years = 0.73, 95%
CI = 0.58 to 0.91, P trend = 0.004). The protective effect of a larger somatotype was found to
be significant (P trend<0.05) for ER-negative, PR-positive and PR-negative subtypes and
marginally significant (P trend = 0.062) for the ER-positive subtype. Within the group
consisting of large somatotypes, the most prominent effects were shown in ER-negative (OR
comparing large to lean somatotype at age seven years = 0.40, 95% CI = 0.21 to 0.75, P trend
= 0.002) and PR-negative (0.63, 95% CI = 0.40 to 0.99, P trend = 0.028) tumours. The point
estimates changed very little before and after additional adjustment for mammographic
density as a continuous variable [see Table S2 in Additional file 2], using a subset of the data
with this information available (n = 3232).
We next assessed the effects of childhood body size on tumour characteristics (ER status, PR
status, tumour size, grade, histology, and absence/presence of metastatic nodes) by fitting
binary/ordinal logistic regression models, adjusting for age at diagnosis in years as a
confounder. We established that the protective effect of somatotype at age seven years was
significantly stronger for ER-negative disease than for ER-positive disease (P heterogeneity =
0.046; Table 3). When comparing between two extreme groups, women with a larger body
size at age seven years were 1.71 times (95% CI = 0.96 to 3.06) more likely to get ER-
positive than ER-negative disease after menopause. Although the estimated trend suggests
that women with the same physique are more likely to get the PR-positive disease in
adulthood, the difference between the two tumour subtypes was not significant (P
heterogeneity = 0.283). The point estimates for tumour size, histology, grade, or the presence
or absence of metastatic nodes did not vary much before and after adjustment for age of
Discussion {1st Level Heading}
Our first main finding was that a large somatotype at age seven years was associated with a
decreased risk of postmenopausal breast cancer. Although strongly associated with other risk
factors such as age of menarche, adult BMI and mammographic density, somatotype at age
seven years remained a significant protective factor (OR comparing large to lean somatotype
at age seven years = 0.73, 95% CI = 0.58 to 0.91, P trend = 0.004) after adjustment for these
other risk factors. Our second and most novel finding was of a significant protective effect of
somatotype at age seven years regardless of receptor status, but with a stronger effect for ER-
negative (0.40, 95% CI = 0.21 to 0.75, P trend = 0.002), than for ER-positive (0.80, 95% CI =
0.62 to 1.05, P trend = 0.062), tumours (P heterogeneity = 0.046).
Our findings regarding the protective effects of childhood body size for adult breast cancer
are consistent with previous studies [3-5]. Associations with other breast cancer risk factors
were also in the same direction as found in other epidemiological studies. Several studies
have found birth weight and gain in BMI in early childhood to predict adult lean mass, while
adult adiposity has been attributed to weight gain in late childhood and adolescence [15-19].
Similarly, anthropometric measurements at other time points (birth weight, and somatotype
one year prior to enrolment) in our data were found to be positively associated with
somatotype at age seven years. The adverse effects of birth weight and adult body mass on
postmenopausal breast cancer risk may be explained by a surplus of estrogen exposure from
either the uterine environment or excess adipose tissue [4, 20]. However, studies performed
on children have not consistently found an association between obesity and circulating
estradiol levels [21, 22], thus it is unclear what mechanisms drive the associated decrease in
risk during the pre-/peri-puberty window.
Strong inverse relationships found between childhood body size, age of menarche, benign
breast disease, and mammographic density were in line with other reports in the literature.
Baer and colleagues [23] found a large childhood body size to be associated with a decrease
in risk of benign breast disease. Age of menarche is often considered along with age of
menopause and other hormonal risk factors for a woman’s cumulative exposure to estrogen
[24, 25]. An earlier age of menarche is associated with an increased risk of breast cancer. On
the other hand, a larger childhood somatotype, which is associated with decreased breast
cancer risk, is also associated with an earlier age of menarche. As age of menarche is an
established but weak predictor of breast cancer risk, its pronounced inverse relationship with
childhood body size when seen in the context of breast cancer risk seems to be
Mammographic density has also been found by others to be associated with childhood body
mass [5]. Estrogen is produced by adipose tissue in the body. A higher BMI is thus correlated
with higher endogenous estrogen levels. In a murine study, exposure to estrogen prior to
puberty led to a decrease in radiologically dense tissue and an increase in the number of
radiolucent structures [28], which may be analogous to a lower mammographic density in
humans. In agreement, McCormack and colleagues [29] showed that high childhood BMI was
associated with a lower Wolfe grade, and Samimi and colleagues [5] found that a rounder pre-
pubertal body shape was predictive of lower mammographic density later in life.
The age-adjusted case-only comparison of our data reflected a significant difference in the
effects of childhood body size on the two ER subtypes (P trend = 0.046), but not the PR
subtypes. However, in lieu of the fact that PR is an estrogen-induced target gene, and that its
presence could serve to indicate ER functional capacity and tumour differentiation state [30],
we also conducted stratified analyses on PR subtypes. We found that the protective trend
conferred by a larger childhood somatotype on postmenopausal breast cancer applies to all
ER and PR tumour subtypes. Overall our results were consistent with Bardia and colleagues
[7], although in that study the effects were only significant for ER-positive (0.80, 95% CI =
0.67 to 0.96) and PR-negative (0.62, 95% CI = 0.43 to 0.89) tumours (comparing women with
above average weight at age 12 years to women with average weight at age 12 years).
Although Bardia and colleagues observed a stronger protective effect in ER-negative tumours
than in their ER-positive counterparts (in agreement with our finding) when comparing
women with above average weight at age 12 years to women with average weight at age 12
years, the association they observed in this subgroup was not statistically significant (0.77,
Hormonal exposure and mammographic density are established risk factors of breast cancer
that have been suggested to be independent, operating through different pathways [31].
Adjustment for these factors and other traditional risk factors did not attenuate the negative
association of childhood body size on breast cancer risk (OR comparing large to lean
somatotype at age seven years = 0.73, 95% CI = 0.58 to 0.91, P trend = 0.004, for association,
after adjustment), thus suggesting an independent underlying mechanism. We speculate that a
possible mechanism driving the negative association with breast cancer risk could be
epigenetic changes that occur during mammary development. Hilakivi-Clarke [32]
summarised in a review several perspectives on special windows of mammary development.
Mammary tissue is postulated to undergo epigenetic extensive modelling or re-modelling
during different stages in life such as fetal development, puberty or pregnancy. Such
epigenetic modification can persist into adulthood if taken place in mammary stem cells,
uncommitted mammary myoepithelial or luminal progenitor cells and inherited by subsequent
daughter cells [33]. Prepubertal exposure to estrogen has been shown to upregulate the
expression of BRCA1, a well-known DNA repair gene [28]. Liu and colleagues [34] also
demonstrated that BRCA1 is responsible for differentiating ER-negative stem/progenitor cells
into ER-positive luminal cells. They also proposed that loss of expression of the DNA repair
gene (BRCA1) may result in an accumulation of ER-negative stem cells with multiple genetic
defects. Incidentally, loss of BRCA1 is frequently associated with ER-negative breast cancers
[35]. The evidence for altered gene expression possibly caused by childhood body size helps
to explain the general reduction in breast cancer risk overall. The apparent differential
protection conferred to the ER-negative subtype could possibly be driven by the same
underlying mechanism that operates through epigenetic modifications.
The strengths of our study include it being a population-based study, its large sample size and
detailed information on many variables: anthropometric measures at different time points
throughout life, mammographic density, reproductive and hormonal risk factors, and tumour
characteristics. To our knowledge, this is the first study to consider the effects of somatotype
at age seven years on adult breast cancer with the consideration of mammographic density,
and also the first to examine its effects on tumour characteristics other than ER status.
A limitation of our study is that risk factor data were self-reported, and could thus be
measured with error. Although two studies have demonstrated the validity of using the nine-
level somatotype diagram for the long-term recall of childhood body size via high correlations
with BMI at the same ages [8, 36], it is noteworthy that in those studies no woman recalled
their figure as larger than level seven in these studies, and that women with large body size
were more likely to misreport their childhood somatotypes than women who were lean.
However, any such measurement error is most likely to attenuate any association between
childhood body size and breast cancer risk [37]. In addition, as the questionnaire study was
conducted post-diagnosis of breast cancer, recall bias could have been introduced. Although
the nine-level somatotype measure has not been validated specifically in a group of breast
cancer cases, it is unlikely that childhood body size was differentially recalled by breast
Conclusions {1st Level Heading}
Our findings may have important implications. The effects of childhood body size on the
different breast cancer subtypes are independent of other breast cancer risk factors, such as
mammographic density and estrogen exposure. Given the strength of the associations, and the
ease of retrieval of information on childhood somatotypes retrospectively from pictures early
in life, childhood body size is potentially useful for building breast cancer risk or prognosis
prediction models. It appears counterintuitive that a large body size during childhood can
reduce breast cancer risk or alter one’s prognosis, because a large birth weight and a high
adult BMI have been shown to otherwise elevate breast cancer risk. There remain unanswered
questions on mechanisms driving this protective effect. Because body size and related
hormonal exposures are modifiable risk factors, women might substantially decrease their risk
of breast cancer, in particular the more aggressive ER-negative disease, by monitoring their
nutrition and exogenous hormone intake at different points in life.
Abbreviations {1st Level Heading}
BMI, body mass index; CI, confidence interval; ER, estrogen receptor; HRT, hormone
replacement therapy; OR, odds ratio; PR, progesterone receptor.
Competing interests {1st Level Heading}
The authors declare no competing interests.
Authors' contributions {1st Level Heading}
JLi participated in the study design, carried out the analyses and drafted the manuscript. LE
digitised and obtained readings for the mammograms. KH, KC, JLiu and PH participated in
study design and coordination and helped to draft the manuscript. All authors read and
Acknowledgements {1st Level Heading}
This work was supported by National Institutes of Health (RO1 CA58427); the Märit and
Hans Rausing's Initiative against Breast Cancer; and the W81XWH-05-1-0314 Innovator
Award, US Department of Defense Breast Cancer Research Program, Office of the
Congressionally Directed Medical Research Programs. J Li is a recipient of the A*STAR
Graduate Scholarship. KH was supported by the Swedish Research Council (523-2006-972).
KC was financed by the Swedish Cancer Society (5128-B07-01PAF). The sponsors took no
role in the study design, the collection or analysis of the data, the interpretation of the results,
the preparation of the manuscript, or the decision to submit the manuscript for publication.
References {1st Level Heading}
Magnusson C, Baron J, Persson I, Wolk A, Bergstrom R, Trichopoulos D, Adami HO:
Body size in different periods of life and breast cancer risk in post-menopausal women.Int J Cancer 1998, 76:29-34.
Hilakivi-Clarke L, Forsen T, Eriksson JG, Luoto R, Tuomilehto J, Osmond C, Barker
DJ: Tallness and overweight during childhood have opposing effects on breast cancer risk.Br J Cancer 2001, 85:1680-1684.
Berkey CS, Frazier AL, Gardner JD, Colditz GA: Adolescence and breast carcinoma risk.Cancer 1999, 85:2400-2409.
Ahlgren M, Melbye M, Wohlfahrt J, Sorensen TI: Growth patterns and the risk of breast cancer in women.N Engl J Med 2004, 351:1619-1626.
Samimi G, Colditz GA, Baer HJ, Tamimi RM: Measures of energy balance and mammographic density in the Nurses' Health Study.Breast Cancer Res Treat
2008, 109:113-122.
Boyd NF, Rommens JM, Vogt K, Lee V, Hopper JL, Yaffe MJ, Paterson AD:
Mammographic breast density as an intermediate phenotype for breast cancer. Lancet Oncol 2005, 6:798-808.
Bardia A, Vachon CM, Olson JE, Vierkant RA, Wang AH, Hartmann LC, Sellers TA,
Cerhan JR: Relative weight at age 12 and risk of postmenopausal breast cancer. Cancer Epidemiol Biomarkers Prev 2008, 17:374-378.
Must A, Willett WC, Dietz WH: Remote recall of childhood height, weight, and body build by elderly subjects.Am J Epidemiol 1993, 138:56-64.
Rosenberg LU, Einarsdottir K, Friman EI, Wedren S, Dickman PW, Hall P,
Magnusson C: Risk factors for hormone receptor-defined breast cancer in postmenopausal women.Cancer Epidemiol Biomarkers Prev 2006, 15:2482-2488.
Orgeas CC, Hall P, Rosenberg LU, Czene K: The influence of menstrual risk factors on tumor characteristics and survival in postmenopausal breast cancer. Breast Cancer Res 2008, 10:R107.
Tamimi RM, Eriksson L, Lagiou P, Czene K, Ekbom A, Hsieh CC, Adami HO,
Trichopoulos D, Hall P: Birth weight and mammographic density among postmenopausal women in Sweden.Int J Cancer 2009, 126:985-991.
Boyd NF, Stone J, Martin LJ, Jong R, Fishell E, Yaffe M, Hammond G, Minkin S:
The association of breast mitogens with mammographic densities.Br J Cancer
2002, 87:876-882.
Bentzon N, During M, Rasmussen BB, Mouridsen H, Kroman N: Prognostic effect of estrogen receptor status across age in primary breast cancer.Int J Cancer 2008, 122:1089-1094.
R Development Core Team: R. A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing; 2005.
Rogers I: The influence of birthweight and intrauterine environment on adiposity and fat distribution in later life.Int J Obes Relat Metab Disord 2003, 27:755-777.
Sachdev HS, Fall CH, Osmond C, Lakshmy R, Dey Biswas SK, Leary SD, Reddy KS,
Barker DJ, Bhargava SK: Anthropometric indicators of body composition in young adults: relation to size at birth and serial measurements of body mass index in childhood in the New Delhi birth cohort.Am J Clin Nutr 2005, 82:456-466.
Sellers TA, Davis J, Cerhan JR, Vierkant RA, Olson JE, Pankratz VS, Potter JD,
Folsom AR: Interaction of waist/hip ratio and family history on the risk of hormone receptor-defined breast cancer in a prospective study of postmenopausal women.Am J Epidemiol 2002, 155:225-233.
Yliharsila H, Kajantie E, Osmond C, Forsen T, Barker DJ, Eriksson JG: Birth size, adult body composition and muscle strength in later life.Int J Obes (Lond) 2007, 31:1392-1399.
Yliharsila H, Kajantie E, Osmond C, Forsen T, Barker DJ, Eriksson JG: Body mass index during childhood and adult body composition in men and women aged 56- 70 y.Am J Clin Nutr 2008, 87:1769-1775.
Friedenreich CM: Review of anthropometric factors and breast cancer risk.Eur J Cancer Prev 2001, 10:15-32.
Klein KO, Larmore KA, de Lancey E, Brown JM, Considine RV, Hassink SG: Effect of obesity on estradiol level, and its relationship to leptin, bone maturation, and bone mineral density in children.J Clin Endocrinol Metab 1998, 83:3469-3475.
Garnett SP, Hogler W, Blades B, Baur LA, Peat J, Lee J, Cowell CT: Relation between hormones and body composition, including bone, in prepubertal children.Am J Clin Nutr 2004, 80:966-972.
Baer HJ, Schnitt SJ, Connolly JL, Byrne C, Cho E, Willett WC, Colditz GA:
Adolescent diet and incidence of proliferative benign breast disease.Cancer Epidemiol Biomarkers Prev 2003, 12:1159-1167.
Emaus A, Espetvedt S, Veierod MB, Ballard-Barbash R, Furberg AS, Ellison PT,
Jasienska G, Hjartaker A, Thune I: 17-beta-estradiol in relation to age at menarche and adult obesity in premenopausal women.Hum Reprod 2008, 23:919-927.
Jansen SC, Temme EH, Schouten EG: Lifetime estrogen exposure versus age at menopause as mortality predictor.Maturitas 2002, 43:105-112.
Cooper C, Kuh D, Egger P, Wadsworth M, Barker D: Childhood growth and age at menarche.Br J Obstet Gynaecol 1996, 103:814-817.
Terry MB, Ferris JS, Tehranifar P, Wei Y, Flom JD: Birth weight, postnatal growth, and age at menarche.Am J Epidemiol 2009, 170:72-79.
Cabanes A, Wang M, Olivo S, DeAssis S, Gustafsson JA, Khan G, Hilakivi-Clarke L:
Prepubertal estradiol and genistein exposures up-regulate BRCA1 mRNA and reduce mammary tumorigenesis.Carcinogenesis 2004, 25:741-748.
McCormack VA, dos Santos Silva I, De Stavola BL, Perry N, Vinnicombe S,
Swerdlow AJ, Hardy R, Kuh D: Life-course body size and perimenopausal mammographic parenchymal patterns in the MRC 1946 British birth cohort.Br J Cancer 2003, 89:852-859.
Hardy DB, Janowski BA, Chen CC, Mendelson CR: Progesterone receptor inhibits aromatase and inflammatory response pathways in breast cancer cells via ligand- dependent and ligand-independent mechanisms.Mol Endocrinol 2008, 22:1812-
Boyd NF, Martin LJ, Sun L, Guo H, Chiarelli A, Hislop G, Yaffe M, Minkin S: Body size, mammographic density, and breast cancer risk.Cancer Epidemiol Biomarkers Prev 2006, 15:2086-2092.
Hilakivi-Clarke L: Nutritional modulation of terminal end buds: its relevance to breast cancer prevention.Curr Cancer Drug Targets 2007, 7:465-474.
De Assis S, Hilakivi-Clarke L: Timing of dietary estrogenic exposures and breast cancer risk.Ann N Y Acad Sci 2006, 1089:14-35.
Liu S, Ginestier C, Charafe-Jauffret E, Foco H, Kleer CG, Merajver SD, Dontu G,
Wicha MS: BRCA1 regulates human mammary stem/progenitor cell fate.Proc Natl Acad Sci U S A 2008, 105:1680-1685.
Karp SE, Tonin PN, Begin LR, Martinez JJ, Zhang JC, Pollak MN, Foulkes WD:
Influence of BRCA1 mutations on nuclear grade and estrogen receptor status of breast carcinoma in Ashkenazi Jewish women.Cancer 1997, 80:435-441.
Must A, Phillips SM, Naumova EN, Blum M, Harris S, Dawson-Hughes B, Rand
WM: Recall of early menstrual history and menarcheal body size: after 30 years, how well do women remember?Am J Epidemiol 2002, 155:672-679.
Gunnell D, Berney L, Holland P, Maynard M, Blane D, Frankel S, Smith GD: How accurately are height, weight and leg length reported by the elderly, and how closely are they related to measurements recorded in childhood?Int J Epidemiol
2000, 29:456-464. Figure legends Figure 1. Nine-level somatotype pictogram. Table 1. Associations of somatotype at age seven years with other breast cancer risk factors (controls only)
* Based on Wald tests for regression coefficients in continuous, ordinal or logistic regression models (see
statistical analyses section). All regression models were adjusted for age at enrolment. † Subset with phenotypic
data. BMI, body mass index; CI, confidence interval; HRT, hormone replacement therapy; OR, odds ratio.
Table 2. Multivariate-adjusted OR estimates and corresponding 95% CIs of postmenopausal breast cancer for somatotype at age seven years, overall and stratified by breast cancer tumour subtype based on ER and PR status
* Logistic regression models were used, accounting for age, age at menarche, benign breast disease and recent
body mass index. CI, confidence interval; ER, estrogen receptor; OR, odds ratio; PR, progesterone receptor.
Table 3. Relation of somatotype at age seven years to tumour-defined characteristics of breast cancer
* Proportional odds logistic regression models were used. † Logistic regression models were used. ‡ Derived
from one degree of freedom trend tests. § Adjusted for age at diagnosis. CI, confidence interval; ER, estrogen
receptor; OR, odds ratio; PR, progesterone receptor.
Additional files Additional file 1
Description: Descriptive characteristics of post-menopausal women.
Additional file 2
Description: Multivariate-adjusted odds ratio (OR) estimates and corresponding 95%
confidence intervals (CIs) of postmenopausal breast cancer for somatotype at age seven years
on a subset of women with mammographic density data; overall and stratified by breast
cancer tumour subtype based on estrogen receptor (ER) and progesterone receptor (PR) status.
Additional files provided with this submission:
Additional file 1: Table S1.doc, 76KAdditional file 2: Table S2.doc, 67K
UC Anschutz Medical Campus Health Sciences Library 12950 E. Montview Blvd., MS A003, Aurora, CO 80045 http://hslibrary.ucdenver.edu/ | AskHSL@lists.ucdenver. edu | 303-724-2152 Ovid Self-Test 1. What are the recent developments in the surgical treatment of morbid obesity in adolescents? 2. What are the effects of working 30 hour shifts on medical residents? 3
Address: Spettgatan 13, 932 32 Skelleftehamn, Sweden Master of Science in Mechanical Engineering. Specialization in Energy Technology University education as upper secondary school Teacher in Mathematics and Physics Upper secondary school degree as Mechanical Engineer Engineer at ABB, ALSTOM Power and SIEMENS PhD student at Luleå Technical University, energy division Teacher at Umeå Un
 Additional files provided with this submission:
Additional files provided with this submission: