Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Hypospadias in males with intrauterine growth restriction due to placental insufficiency: the placental role in the embryogenesis of male external genitalia
Hypospadias in Males With Intrauterine GrowthRestriction Due To Placental Insufficiency:The Placental Role in the Embryogenesis ofMale External GenitaliaYoav Yinon,1 John C.P. Kingdom,1 Leslie K. Proctor,1 Edmond N. Kelly,2 Joao L. Pippi Salle,3Diane Wherrett,4 Sarah Keating,5 Ori Nevo,6 and David Chitayat7*1Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, The Placenta Clinic, Mount Sinai Hospital, University of Toronto,Toronto, Ontario, Canada2Department of Pediatrics, Neonatal Intensive Care Unit, Mount Sinai Hospital, University of Toronto, Toronto, Ontario, Canada3Department of Pediatric Urology, The Hospital for Sick Children, University of Toronto, Toronto, Ontario, Canada4Division of Endocrinology, Department of Pediatrics, The Hospital for Sick Children, University of Toronto, Toronto, Ontario, Canada5Department of Pathology and Laboratory Medicine, Mount Sinai Hospital, University of Toronto, Toronto, Ontario, Canada6Department of Obstetrics and Gynecology, Sunnybrook Health Centre, University of Toronto, Toronto, Ontario, Canada7The Prenatal Diagnosis and Medical Genetics Program, Mount Sinai Hospital, University of Toronto, Toronto, Ontario, Canada
Received 20 August 2009; Accepted 11 September 2009
Our aim was to define the association between early onset intra-
uterine growth restriction (IUGR) due to placental insufficiency
Yinon Y, Kingdom JCP, Proctor LK, Kelly EN,
and hypospadias in males. We prospectively studied a cohort of
Pippi Salle JL, Wherrett D, Keating S, Nevo O,
small-for-gestational age (SGA) male infants with hypospadias
Chitayat D. 2010. Hypospadias in males with
managed by a multidisciplinary team over a 5-year period. Thirty
SGA male infants were diagnosed with hypospadias/abnormal
placental insufficiency: The placental role in
genitalia after birth, and four of them were diagnosed antena-
the embryogenesis of male external genitalia.
tally. Five cases occurred in the smaller pair of discordant IUGR
twins, where the larger co-twin had normal male genitalia. Serialultrasounds demonstrated features of early-onset IUGR in allcases at a median gestational age of 21 weeks (range 14–31weeks). Twenty-one (70%) pregnancies were subsequently complicated
Key words: placental insufficiency; intra-uterine growth restric-
by absent/reversed end-diastolic flow in the umbilical arteries
indicating severe IUGR, and 17 (57%) women developed severepre-eclampsia. There were 27 (90%) live births at a mediangestational age of 31 weeks (range 27–37); 23 (77%) of the
neonates had birth weights <3rd centile. All newborns hadnormal male karyotypes. In 62% (18/29) the hypospadias was
Hypospadias is a common malformation in males with an incidence
severe. A correlation was found between the severity of the
of 0.3–0.4% [Gallentine et al., 2001; Brouwers et al., 2007]. It results
IUGR and the severity of hypospadias as significantly more
from an incomplete fusion of the urethral folds between the 7th and
infants with severe hypospadias were less than the 3rd centilecompared to the mild–moderate hypospadias group: 94% (17/18) versus 55% (6/11), respectively (P ¼ 0.02). In conclusion,
*Correspondence to:David Chitayat, Department of Obstetrics and Genecology, The Prenatal
SGA male newborns with hypospadias exhibit a high rate of early
Diagnosis and Medical Genetics Program, The Ontario Power Generation
-onset severe IUGR due to placental insufficiency. Early placental
Building, 700 University Avenue, Room 3292, Toronto, Ontario, Canada
development likely influences male external genitalia formation.
Careful sonographic evaluation of the genitalia is advised when
Published online 11 December 2009 in Wiley InterScience
early-onset placentally mediated IUGR is found.
AMERICAN JOURNAL OF MEDICAL GENETICS PART A
14th week of gestation. Most cases are isolated and are presumed to
[Viero et al., 2004; Toal et al., 2008]. After delivery, all placentas
be multifactorial traits [Calzolari et al., 1986; Baskin et al., 2001;
were examined pathologically, including assignment of chorionic-
Manson and Carr, 2003]. Previous epidemiologic studies found a
close relationship between low birth weight and hypospadias
Antenatal data were collected prospectively and included ma-
[Calzolari et al., 1986; Akre et al., 1999; Weidner et al., 1999], yet
ternal demographic information (age, race, parity, exposure to
the underlying mechanism of this association is unclear. Hussain
alcohol, tobacco, substance abuse and other teratogens, and pre-
et al. [2002] demonstrated that hypospadias was significantly more
existing chronic diseases), mode of conception, first and second
common in infants who were small-for-gestational age (SGA),
trimester screening as well as fetal karyotype determined by am-
suggesting that intra-uterine growth restriction (IUGR) rather than
niocentesis, serial ultrasound findings, and obstetrical complica-
the absolute birth weight is a more important risk factor for
tions. Hypertensive disorders were defined according to the
hypospadias. Some evidence suggests that placental insufficiency
American College of Obstetricians and Gynecologist criteria
may be the underlying factor, for example, hypospadias correlates
[ACOG, 2002]. Delivery information was reviewed and included
with low weight of the placenta [Stoll et al., 1990], and has been
birth weight, gestational age at delivery, Apgar scores, head cir-
observed in the smaller twin in a mono-chorionic twin pregnancy
cumference and length at birth, genital findings, neonatal compli-
complicated by discordant growth [Fredell et al., 1998]. These data
cations, and placental histopathology.
suggest that the association of low birth weight with hypospadias
A diagnosis of hypospadias was based on an initial physical
may be related to placental dysfunction. Since the most severe forms
examination; confirmation of diagnosis and severity grading were
of IUGR have their origins in the first trimester [Smith et al., 1998],
done by a pediatric urologist. The severity of hypospadias was based
we tested the hypothesis that severe hypospadias is associated with
on the anatomical position of the urethral meatus: glandular,
early-onset severe placental insufficiency.
coronal, and penile were defined as mild–moderate and penoscro-tal, scrotal and perineal were defined as severe [Boisen et al., 2005].
The evaluation of these infants included abdominal ultrasonogra-phy to define the internal genitalia, chromosome analysis, and
Institutional research ethics board approval was obtained to audit
extensive endocrinology work-up in cases of ambiguous genitalia,
clinical outcomes and relate these to screening tests of placental
which included blood testosterone level, 17-OH progesterone, FSH,
LH, thyroid function tests, dehydrotestosterone, cortisol, andro-
Between 2004 and 2008, 1,659 preterm male infants were born at
stenedione, DHEAS, and sex hormone binding globulin levels.
Mount Sinai Hospital, 156 of them were SGA and consisted of our
Some of the cases had DNA analysis of the androgen receptor and
study cohort. Out of this cohort, all male infants who were diag-
7-dehydrocholesterol. All the patients had serial follow-up in the
nosed with hypospadias/abnormal genitalia after birth were iden-
neonatal neurodevelopmental and pediatric urology clinics.
tified. They all underwent a multidisciplinary assessment and care
Descriptive statistics are presented as mean Æ 1 SD or median
by a team consisting of geneticists, endocrinologists, neonatolo-
(range). Fisher’s exact test was used for statistical comparison of
gists, and pediatric urologists. All cases of IUGR and hypospadias
categorical variables. A P-value <0.05 was considered significant.
were followed antenatally in our multidisciplinary placenta clinic,six of them were referred prior to delivery. In this clinic, we screen
and follow pregnancies that are considered to be high risk because ofmedical or obstetric complications for placental dysfunction. This
Thirty SGA male infants were diagnosed with hypospadias/abnor-
includes first trimester screening at 10–13 weeks of gestation,
mal genitalia after birth during the 5-year period. Maternal demo-
maternal serum screening at 16–18 weeks, and placental ultrasound
graphic data and pregnancy characteristics of these cases are shown
examination with uterine artery Doppler evaluation at 19–23
in Table I. Twenty-three (77%) of these pregnancies were conceived
weeks. Pregnancy-associated plasma protein-A (PAPP-A) levels
spontaneously, the remainder were conceived following ovulation
<0.3 multiples of the median (MoM) and alpha-fetoprotein (AFP)
induction via clomiphene citrate (1), gonadotropins (3), or in vitro
>2.0 MoM were considered abnormal as previously reported
fertilization (3). Five were the smaller IUGR co-twin in discordant
[Alkazaleh et al., 2006]. Once a diagnosis of IUGR due to placental
twins (three were monochorionic-diamniotic, two dichorionic-
insufficiency was made, ultrasound examinations were performed
every 2 weeks from 24 weeks of gestation, and increased up to 3 per
Antenatal evidence of placental dysfunction was common; low
week depending on the gestational age, severity of IUGR
PAPP-A levels <0.3 MoM were found in 45% and elevated AFP
(determined by fetal Doppler studies, biophysical profile scores,
>2.0 MoM in 71%. Both markers were abnormal in 36% of cases.
and amniotic fluid volume), and the presence/severity of pre-
Abnormal uterine artery Doppler (mean pulsatility index >1.45
eclampsia. Sonographic findings indicating placental insufficiency
and bilateral early diastolic notches) was found in 50% (11/22) of
were recorded including absent or reversed end-diastolic flow
pregnancies that had performed this test.
velocities (AREDV) in the umbilical arteries; elevated head/abdo-
Serial ultrasound examinations established the diagnosis of early
men circumference ratio above the 95th centile for gestational age
onset of growth restriction by the defined criteria at a median
indicating asymmetrical IUGR [Snijders and Nicolaides, 1994];
gestational age of 21 weeks. Sonographic findings indicating pla-
reduced amniotic fluid volume (amniotic fluid index <5 cm);
cental dysfunction consisted of absent/reversed end-diastolic flow
abnormal placental shape (small/thick) and texture; bilateral ab-
in the umbilical arteries in 21 (70%) fetuses, oligohydramnios in 15
normal uterine artery Doppler, both as we have previously defined
(50%) pregnancies, asymmetrical pattern of growth restriction as
TABLE I. Baseline and Pregnancy Characteristics
TABLE II. Obstetrical and Neonatal Outcome
aOnly cases, which resulted in live birth, were included.
bAt 18, 27, and 28 weeks of gestation.
villous maturation, perivillous fibrin deposition, decidual vascul-
opathy, infarction, and fetal thrombotic vasculopathy.
Postnatal genitalia findings are summarized as individual cases
In four cases the genital abnormality was diagnosed antenatally
(Fig. 1). In two cases a diagnosis of a female fetus was made and only
after a male karyotype was found by amniocentesis, the diagnosis of
abnormal genitalia was established. Chromosome analysis was
performed postnatally on peripheral blood lymphocytes and all
showed a normal male karyotype (46, XY). In 11, the karyotype was
determined prenatally in amniocytes and confirmed after birth.
Severe proximal hypospadias occurred in 62% (18/29) of the
aThree monochorionic-diamniotic and two dichorionic-diamniotic twins.
newborns and mild–moderate hypospadias was seen in 38% (11/29). Of the 18 infants with severe hypospadias, 17 (94%) were belowthe 3rd centile compared to 6 (55%) infants with mild–moderatehypospadias (P ¼ 0.02). The incidence of AREDV in the umbilical
evident by head/abdomen circumference ratio above the 95th
artery was similar in both groups: 67% (12/18) in the severe
centile in 15 fetuses (50%), and abnormal placental shape or texture
hypospadias group versus 82% (9/11) in the mild hypospadias
group (P ¼ 0.7). Associated genital abnormalities included micro-
The obstetrical and neonatal outcomes are summarized in
Table II. Of the 30 pregnancies, 27 (90%) were live born at amedian gestational age of 31 weeks (range 27–37 weeks). Pretermdelivery at <34 weeks of gestation occurred in 28 women (93%); all
TABLE III. Histopathologic Findings of the Placenta
were iatrogenic by induction of labor or by cesarean section for thefollowing reasons: severe pre-eclampsia (14), severe IUGR
(accompanied by pre-eclampsia in two of them), and non-
reassuring fetal condition by ultrasound and/or non-stress test
(9), placental abruption (2), intra-uterine fetal death (IUFD)
(2), and pre-eclampsia with IUFD (1).
Mean birth weight was 970 g (range 460–2,195); 23 (77%) of the
neonates were below the 3rd centile for sex and gestational age
according to birth weight data for Canadian infants [Kramer et al.,
2001], and the rest were below the 10th centile.
The placental histopathologic findings are summarized in
Table III. Twelve (45%) had a small placenta (weight <10th
centile). Findings consistent with ischemic–thrombotic placental
aPlacental pathology was not available for three cases.
pathology were found in 22 (81%) cases including accelerated
AMERICAN JOURNAL OF MEDICAL GENETICS PART A
AMERICAN JOURNAL OF MEDICAL GENETICS PART A
(regarding the possibility of partial androgen insensitivity) wasperformed. At the completion of these investigations a male genderwas assigned in all cases, and none of them had evidence ofincomplete androgen insensitivity.
Three of the cases had non-genital anomalies: the first was a
patient with hydrocephalus, minor facial anomalies, and clinodac-tyly of the 5th fingers, feeding difficulties and developmental delaywho died at the age of 9 months. The second was a neonate who wasborn at 28 weeks gestation, weighed 570 g and had facial anomalies,and died 5 min after birth. The third was a patient with Ebsteinanomaly and coarctation of the aorta who died in utero at 18 weeksof gestation. In all three extensive investigations were done but nospecific diagnosis could be made. The possibility that the hypo-sdpadias was secondary to a syndrome in these three cases could notbe excluded.
Our cohort included five sets of discordant twins, in which the
IUGR twin had hypospadias and the healthy co-twin had normalmale genitalia (Table III, cases 15–19). Three of these twins weremonochorionic-diamniotic and all were complicated with severepre-eclampsia. Interestingly, the severity of the hypospadias ap-peared to be milder in the IUGR twins: four of the five IUGR twinshad mild hypospadias, whereas only 7 of the 25 IUGR singletonshad mild hypospadias.
This study describes the association between hypospadias and earlyonset IUGR in 30 fetuses over a 5-year-time period in a single center. This cohort of patients is unique as all had antenatal follow-upshowing early onset of IUGR with sonographic findings indicatingsevere placental dysfunction in most of these pregnancies. More-over, our cohort represents the more extreme cases of IUGR as mostof the fetuses (77%) were below the 3rd centile. The nature andseverity of the underlying placental disease was substantiated bypostnatal histopathologic examination of the placentas by a peri-natal pathologist. Nearly half had chorion regression (small pla-centas with eccentric cords) [Proctor et al., 2009] and most hadsome evidence of ischemic–thrombotic injury to the gas-exchang-ing placental villi. Of these infants, 62% had severe hypospadias and11 had ambiguous genitalia. All these infants had normal malekaryotypes, and none had evidence of an underlying genetic causefor hypospadias.
The association between low birth weight and hypospadias has
been described before [Calzolari et al., 1986; Akre et al., 1999;Weidner et al., 1999], and two previous studies have reported on theassociation between IUGR and hypospadias [Hussain et al., 2002;Fujimoto et al., 2008]. However, in these studies a diagnosis of
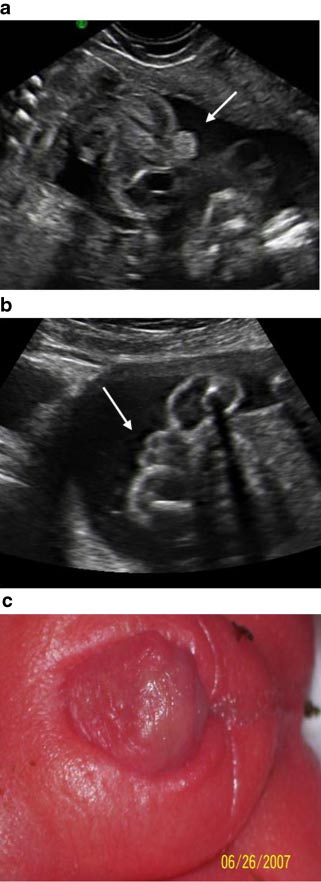
FIG. 1. Ultrasound image at 28 weeks of gestation of an IUGR fetus
IUGR was inferred due to a postnatal diagnosis of SGA infant at
with AEDV demonstrating micropenis, hypospadias (a), and bifid
birth. Our study progresses the findings of these earlier reports by
scrotum (b); postnatal examination confirmed the antenataldiagnosis (c). [Color figure can be viewed in the online issue, which
establishing a clear link both to severely impaired fetal growth and
is available at www.interscience.wiley.com.]
to an underlying diagnosis of severe placental dysfunction. Fetalgrowth restriction can result from a variety of intrinsic or extrinsic
penis (8), bifid scrotum (9), penoscrotal transposition (6), severe
insults, yet all our cases had sonographic findings indicating
chordee (11), and cryptorchidism (14).
placental dysfunction as the cause of growth restriction.
In 11 infants the hypospadias was so severe that the gender could
Hussain et al. showed a 3.83% incidence of hypospadias among
not be determined. All were investigated by our Multidisciplinary
SGA male infants compared to 1.27% among AGA infants [Hussain
Urogenital Team, and DNA analysis of the androgen receptor gene
et al., 2002]. Recently, Fujimoto et al. reported on a series of 104
AMERICAN JOURNAL OF MEDICAL GENETICS PART A
extremely low birth weight (<1,500 g) male infants, and 16 (15.3%)
female external genitalia. An alternative explanation is that one or
of them having hypospadias [Fujimoto et al., 2008]. Our study
more of the growing array of genes controlling early fate decisions in
design is not able to determine the true incidence of hypospadias
placentation [Rawn and Cross, 2008] either directly or indirectly
among IUGR fetuses due to the inherent selection bias in our
affects the formation of the male external genitalia.
tertiary clinical practice. However, since during the study period,
A large proportion (62%) of the infants in our study had severe
156 IUGR male infants less than 37 weeks of gestation were
hypospadias compared to only 6% in the Fredell et al. cohort of
delivered at our hospital, the rough estimate for the incidence of
2,500 boys with hypospadias [Fredell et al., 2002] and 23% in
hypospadias in IUGR fetuses is 19% (30/156) compared to a
Hussain’s study, which included SGA infants with hypospadias
background incidence of 0.3% [Gallentine et al., 2001; Brouwers
[Hussain et al., 2002]. This may reflect the early onset as well as the
et al., 2007]. Therefore, it is likely that severe placental dysfunction
severity of the placental dysfunction in our cohort of patients, in
is causally associated with disruption of normal male external
view of the fact that our center is a tertiary facility involved in the
genital development. During the study period no case of term
more severe cases of IUGR. Unlike previous studies, which did not
IUGR with hypospadias was identified, indicating that this associa-
show a correlation between the severity of hypospadias and the
tion is more common among the severe cases of growth restriction,
severity of growth restriction [Hussain et al., 2002; Fujimoto et al.,
2008], our data do support such relationship as significantly more
In the Fujimoto et al. [2008] study, 16 male infants with
infants with severe hypospadias were below the 3rd centile com-
hypospadias and birth weight below 1,500 g were compared to
pared to the ones with mild–moderate hypospadias.
62 controls whose birth weight was less than 1,500 g but did not have
Another indication for an association between IUGR and hy-
hypospadias. The patients with hypospadias demonstrated a sig-
pospadias comes from monozygotic twins. A study of 18 twin pairs
nificantly higher placenta-to-fetal ratio associated with placental
in which one twin had hypospadias and one did not, found that in
infarction compared to controls [Fujimoto et al., 2008]. Moreover,
16 pairs, the healthy co-twin weighed at birth 500 g more than the
placental histopathologic findings in the hypospadias cases revealed
twin with hypospadias [Fredell et al., 1998]. In our study five of the
severe degenerative changes, infarction, and calcification, similar to
cases were twins (three monochrionic and two dichorionic with
the findings in our study. However, the prevalence of pregnancy-
unknown zygosity), in which the IUGR twin was the one with
induced hypertension in their study was significantly lower in the
hypospadias. Since monozygotic twins share the same intrauterine
hypospadias group than in controls (14.2% vs. 26%, respectively),
environment and genotype as well as the same placenta, the
whereas 57% of the pregnancies in our series were complicated by
discordance for the hypospadias is difficult to explain. Conditions,
severe pre-eclampsia, as expected in the presence of severe placental
for which monozygotic twins are discordant, are usually multifac-
dysfunction. Similarly, in a large population-based case-control
torial or the result of a new dominant mutation that affected one of
study hypospadias was shown to be associated with severe pre-
the twins or discordance for a chromosome abnormality, which was
eclampsia with an odds ratio of 2.1 [Akre et al., 1999]. The
ruled out in our cases. However, these data support the hypothesis
association between pre-eclampsia and hypospadias reflects abnor-
that fetal growth and risk of hypospadias are strongly associated and
may indicate an epigenetic phenomena as the cause of the associa-
The most severe forms of placenta-mediated IUGR originate in
the early part of the first trimester, around weeks 7–8, when the male
Since there is substantial evidence for increased risk of
external genitalia are forming. This has been supported by studies
hypospadias/ambiguous genitalia in IUGR male fetuses, in patients
showing that low maternal circulating levels of PAPP-A at 8–14
with early placental dysfunction an US study directed to the fetal
weeks of gestation are significantly predictive of IUGR, and more so
genitalia should be considered, and if amniocentesis is done
when measured prior to 13 weeks [Smith et al., 2002, 2006; Dugoff
correlation between the fetal phenotypic sex and chromosome sex
et al., 2004]. However, the underlying mechanism of the association
should be determined. A discrepancy between the two should be
between hypospadias and placental insufficiency is unclear. The
discussed among the specialists involved in the investigation and
development of the human male urethra, which occurs between 7
treatment of babies with ambiguous genitalia and presented to the
and 14 weeks of gestation, is the result of androgen action on the
women/couples in view of the above findings. This will allow the
external genitalia. Lack of testosterone, 5-alpha reductase deficien-
women/parents to make an informed decision regarding the preg-
cy, complete or incomplete androgen receptor insensitivity, and
nancy and to prepare them for the delivery and the postnatal
steroidogenic enzyme deficiencies are known to result in ambigu-
investigation and treatment required. An attempt should be made
ous genitalia. The earlier the disruption, the more severe the
to obtain a piece of cord and cord blood to allow in depth postnatal
hypospadias [Main et al., 2006]. Since fetal testosterone secretion
investigation since obtaining sufficient amount of blood for DNA
is under the influence of placental hCG during the first 14 weeks of
extraction, in these cases, may be difficult.
gestation [Brouwers et al., 2007], placental dysfunction leading toinsufficient hCG supply, may theoretically result in hypospadias[Fredell et al., 2002]. However, placental dysfunction is known to be
associated with high maternal serum hCG. Thus, it seems that thereis another placental enzyme involved in normal placental function,
ACOG Practice bulletin. Number 33, January. 2002. Diagnosis and man-
which also produces androgens, necessary for the normal develop-
agement of preeclampsia and eclampsia. Obstet Gynecol 99:159–167.
ment of male external genitalia. This mechanism may be similar to
Akre O, Lipworth L, Cnattingius S, Sparen P, Ekbom A. 1999. Risk factor
the placental esterase deficiency that causes masculinization of the
patterns for cryptorchidism and hypospadias. Epidemiology 10:364–369.
Alkazaleh F, Chaddha V, Viero S, Malik A, Anastasiades C, Sroka H,
Kramer MS, Platt RW, Wen SW, Joseph KS, Allen A, Abrahamowicz M,
Chitayat D, Toi A, Windrim RC, Kingdom JC. 2006. Second-trimester
Blondel B, Breart G. 2001. A new and improved population-based
prediction of severe placental complications in women with combined
Canadian reference for birth weight for gestational age. Pediatrics
elevations in alpha-fetoprotein and human chorionic gonadotrophin.
Main KM, Jensen RB, Asklund C, Hoi-Hansen CE, Skakkebaek NE. 2006.
Baskin LS, Himes K, Colborn T. 2001. Hypospadias and endocrine
Low birth weight and male reproductive function. Horm Res 65:116–122.
disruption: Is there a connection? Environ Health Perspect 109:
Manson JM, Carr MC. 2003. Molecular epidemiology of hypospadias:
Review of genetic and environmental risk factors. Birth Defects Res Part A
Boisen KA, Chellakooty M, Schmidt IM, Kai CM, Damgaard IN, Suomi
AM, Toppari J, Skakkebaek NE, Main KM. 2005. Hypospadias in a cohort
Proctor LK, Toal M, Keating S, Chitayat D, Okun N, Windrim RC, Smith
of 1072 Danish newborn boys: Prevalence and relationship to placental
GC, Kingdom JC. 2009. Placental size and the prediction of severe early-
weight, anthropometrical measurements at birth, and reproductive
onset intrauterine growth restriction in women with low pregnancy-
hormone levels at three months of age. J Clin Endocrinol Metab
associated plasma protein-A. Ultrasound Obstet Gynecol 34:274–282.
Brouwers MM, Feitz WF, Roelofs LA, Kiemeney LA, de Gier RP, Roeleveld
Rawn SM, Cross JC. 2008. The evolution, regulation, and function of
N. 2007. Risk factors for hypospadias. Eur J Pediatr 166:671–678.
placenta-specific genes. Annu Rev Cell Dev Biol 24:159–181.
Calzolari E, Contiero MR, Roncarati E, Mattiuz PL, Volpato S. 1986.
Smith GC, Smith MF, McNay MB, Fleming JE. 1998. First-trimester growth
Aetiological factors in hypospadias. J Med Genet 23:333–337.
and the risk of low birth weight. N Engl J Med 339:1817–1822.
Dugoff L, Hobbins JC, Malone FD, Porter TF, Luthy D, Comstock CH,
Smith GC, Stenhouse EJ, Crossley JA, Aitken DA, Cameron AD, Connor
Hankins G, Berkowitz RL, Merkatz I, Craigo SD, Timor-Tritch IE, Carr
JM. 2002. Early pregnancy levels of pregnancy-associated plasma protein
SR, Wolfe HM, Vidaver J, D’alton ME. 2004. First-trimester maternal
a and the risk of intrauterine growth restriction, premature birth,
serum PAPP-A and free-beta subunit human chorionic gonadotropin
preeclampsia, and stillbirth. J Clin Endocrinol Metab 87:1762–1767.
concentrations and nuchal translucency are associated with obstetric
Smith GC, Shah I, Crossley JA, Aitken DA, Pell JP, Nelson SM, Cameron
complications: A population-based screening study (the FASTER Trial).
AD, Connor MJ, Dobbie R. 2006. Pregnancy-associated plasma protein A
Am J Obstet Gynecol 191:1446–1451.
and alpha-fetoprotein and prediction of adverse perinatal outcome.
Fredell L, Lichtenstein P, Pedersen NL, Svensson J, Nordenskjold A. 1998.
Hypospadias is related to birth weight in discordant monozygotic twins. J
Snijders RJ, Nicolaides KH. 1994. Fetal biometry at 14–40 weeks’ gestation.
Ultrasound Obstet Gynecol 4:34–48.
Fredell L, Kockum I, Hansson E, Holmner S, Lundquist L, Lackgren G,
Stoll C, Alembik Y, Roth MP, Dott B. 1990. Genetic and environmental
Pedersen J, Stenberg A, Westbacke G, Nordenskjold A. 2002. Heredity of
factors in hypospadias. J Med Genet 27:559–563.
hypospadias and the significance of low birth weight. J Urol 167:
Toal M, Keating S, Machin G, Dodd J, Adamson SL, Windrim RC,
Kingdom JC. 2008. Determinants of adverse perinatal outcome in high
Fujimoto T, Suwa T, Kabe K, Adachi T, Nakabayashi M, Amamiya T. 2008.
-risk women with abnormal uterine artery Doppler images. Am J Obstet
Placental insufficiency in early gestation is associated with hypospadias. J
Viero S, Chaddha V, Alkazaleh F, Simchen MJ, Malik A, Kelly E, Windrim
Gallentine ML, Morey AF, Thompson IM Jr 2001. Hypospadias: A con-
R, Kingdom JC. 2004. Prognostic value of placental ultrasound in
temporary epidemiologic assessment. Urology 57:788–790.
pregnancies complicated by absent end-diastolic flow velocity in theumbilical arteries. Placenta 25:735–741.
Hussain N, Chaghtai A, Herndon CD, Herson VC, Rosenkrantz TS,
McKenna PH. 2002. Hypospadias and early gestation growth restriction
Weidner IS, Moller H, Jensen TK, Skakkebaek NE. 1999. Risk factors for
in infants. Pediatrics 109:473–478.
cryptorchidism and hypospadias. J Urol 161:1606–1609.
Eidgenössisches Departement des Innern EDI Bundesamt für Gesundheit BAG Direktionsbereich Öffentliche Gesundheit Questions récurrentes sur les médicaments antiviraux contre la grippe pandémi- que (H1N1) 2009 Etat le 27 juillet 2009 à 9 heures Les personnes présentant des symptômes grippaux ou ayant été en contact avec un cas présumé de grippe pandémique (H1N1) doivent-
Helmut Erich SEGNER Born 10th September 1954 in Tauberbischofsheim, GermanyNationality: GermanProfessional address:Centre for Fish and WildlifeUniversity BernPostbox 8466CH-3001 BernTel. +41-31 631 2441/2465, Fax +41-31 631 2611, Email: helmut.segner@itpa.unibe.ch ACADEMIC AND PROFESSIONAL QUALIFICATIONS Habilitation in Zoology, University Karlsruhe: “Morphology, biochemistryand environme
 (regarding the possibility of partial androgen insensitivity) wasperformed. At the completion of these investigations a male genderwas assigned in all cases, and none of them had evidence ofincomplete androgen insensitivity.
(regarding the possibility of partial androgen insensitivity) wasperformed. At the completion of these investigations a male genderwas assigned in all cases, and none of them had evidence ofincomplete androgen insensitivity.