Le tadalafil possède une affinité marquée pour la PDE5, mais épargne en grande partie les isoformes PDE1, PDE2 et PDE11, réduisant ainsi le risque d’effets extra-caverneux. L’action se traduit par une augmentation contrôlée de la circulation sanguine locale, indépendante des variations alimentaires. Sa pharmacocinétique repose sur une absorption digestive rapide, un métabolisme hépatique par CYP3A4 et une distribution tissulaire large. La biodisponibilité reste stable, et l’équilibre plasmatique est atteint en quelques jours lors d’administrations répétées. Les interactions cliniquement significatives surviennent avec les inhibiteurs puissants de CYP3A4 tels que le kétoconazole. Dans la littérature pharmacologique, acheter cialis 20 mg est souvent associé à des schémas d’utilisation basés sur la durée prolongée de son action.
Redcross.org
J O U R N A L O F B L O O D G R O U P S E R O L O G Y A N D E D U C A T I O N
V O L U M E 1 6 , N U M B E R 3 , 2 0 0 0
J O U R N A L O F B L O O D G R O U P S E R O L O G Y A N D E D U C A T I O N
A review: modification of the red blood ce ll membrane and its application in blood group serology Key Words: red cell antigens,enzymes,modification of
able for use in the blood bank. These included plant-
derived proteases: namely, papain extracted frompapaya, ficin extracted from figs, and bromelin extracted
Introduction
from pineapples: and pronase which was isolated from
Blood group antigens are carried on proteins and car-
the culture supernate of Streptomyces griseus (reviewed
bohydrates located on the extracellular surface of the
red blood cell (RBC) membrane.The RBC membrane is
Proteases have been traditionally used to enhance
composed of a lipid bilayer, through which a number of
detection of Rh and Kidd system antibodies, enhance-
proteins pass or are anchored. Proteins bearing blood
ment that results primarily from cleavage of sialic acid-
group antigens vary widely in their structure and func-
bearing glycophorin A and glycophorin B. However, the
tion. Some proteins (e.g., glycophorin C, band 3) are
expansion of knowledge regarding the proteins that
anchored to the intracellular membrane skeleton and
bear the different human blood groups has made the
play a role in maintaining red cell shape and integrity;
action of proteases more valuable in routine serologic
others are transport proteins for specific molecules
tests. Proteases cleave proteins at defined sites along a
(e.g., urea transporter, channel-forming integral protein),
linear peptide sequence, and as such may be used to
and other proteins are receptors (e.g., the LW, Lutheran
modify the RBC antigen expression. Blood group anti-
and Fy glycoproteins) and play a role in cell–cell inter-
gens that are above the enzyme cleavage site on a pro-
tein will be removed following treatment of the RBCs
Blood group antigens may be simple linear sequences
of amino acids (with or without any associated sugarmolecules), or may be formed by the secondary and/ortertiary conformation of the protein.Antigens such as A,B, H, I, and P are entirely carbohydrate, but the oligosac-
charides on which they are carried are attached to pro-teins and lipids of the RBC membrane.
Proteins may be modified by the action of certain
enzymes and chemicals.The action of different modifierson proteins that carry blood group antigens may be usedselectively in antibody identification and may eliminatethe need to test rare RBCs.
Proteases have been used in blood group serology
since 1947, when Morton and Pickles showed that
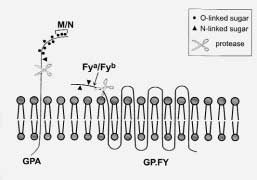
Fig. 1. Effect of proteases: Antigens located above an enzyme-
enzyme solutions obtained from culture extracts of
cleavag site will be removed when RBCs are treated
Vibrio cholerae (sialidase) or from hog stomach
with enzymes. Much of the sialic acid on the RBC also will be removed by protease treatment as these oligosaccharides are
(trypsin) could be used to enhance agglutination reac-
attached to the N-terminal portions of the glycophorins A, B, and
tions. Other sources of proteases were shown to be suit-
Although proteases are more commonly used in
blood group serology, glycosidases (enzymes that cleavesugars) also may help determine an antigen’s character-istics.Table 1 lists the most commonly used enzymes andtheir substrates. Chemical Modification
Chemicals such as dithiothreitol (DTT) and 2-
aminoethylisothiouronium bromide disrupt the sec-ondary structure of polypeptides by reducing the dou-ble bonds between cysteine residues.These bonds formunder oxidizing conditions between the sulfhydrylgroups of cysteine residues in close spatial proximitywithin a protein and give the protein its secondary struc-
ture.6 Many antibodies to blood group antigens recog-
The mechanism by which CDP modifies RBC mem-
nize conformational epitopes; thus, disruption of the sec-
brane proteins is not understood. However, chloroquine
ondary structure of blood group proteins on the RBC
is known to cleave or inhibit noncovalent antigen-anti-
surface will result in the failure of the specific antibody
body binding and is used in that context to remove IgG
to react (Fig. 2). Blood group-bearing proteins that are
bound in vivo from the RBCs of patients with autoim-
sensitive to reducing agents include Kell, Dombrock,
mune hemolytic anemia.9 CDP is known to inactivate Bg
Knops, Lutheran, Indian, Cromer, JMH,AnWj,Yt, LW, and
antigens on RBCs.10 Bg antigens were shown to be HLA
Scianna. Antigens on these proteins may show variable
antigens and were originally thought to have been
susceptibility to DTT treatment. Within the Kell blood
adsorbed from the plasma. Although most RBCs do not
group system, Jsa and Jsb are exquisitely sensitive to
express HLA antigens, Giles et al.11 determined that Bg
reducing agents and are denatured by as little as 1 to 2
antigens are residual HLA class I antigens that are nor-
mM DTT. Other Kell antigens require a concentration of
mally lost upon maturation to the erythrocyte. CDP
specifically removes β-2-microglobulin, part of the het-
ZZAP reagent (marketed as W.A.R.M.; Immucor, Inc.,
erodimer that composes class I HLA antigens, and thus
Norcross, GA) is a mixture of papain and DTT, and incor-
interferes with the conformation of the HLA molecule.11
porates the modification properties of both reagents.7,8ZZAP reagent is commonly used for removing boundIgG from DAT-positive RBCs prior to autoadsorption. However, it also can be used as a one-step treatment ofRBCs as an aid in antibody identification. Table 1: Enzymes commonly used in blood group serology4,20
arginine, lysine, glutamine, tyrosine, glycine, histidine, (next but one to) phenylalanine
arginine, lysine, glutamine, tyrosine, glycine, asparagine, leucine, valine
arginine, lysine, tyrosine, glycine, serine, phenylalanine
phenylalanine, tryptophan, tyrosine, leucine
tyrosine, glycine, leucine, valine, alanine, isoleucine, tryptophan, phenylalanine
α2➝3 and α2➝6 linkages between neuraminic acid and galactose
Note: Proteases hydrolyze the C-terminal bonds of amino acids. References
1. Telen MJ. Erythrocyte blood group antigens: not so
simple after all. Blood 1995;85:299–306.
13. Mallory D, Reid M. Misleading effects of chloroquine
2. Daniels G. Functional aspects of red cell antigens.
14. Louie JE, Jiang AF, Zaroulis CG. Preparation of intact
3. Cartron JP, Bailly P, Le Van Kim C, et al. Insights into
antibody-free red blood cells in autoimmune
the structure and function of membrane polypep-
hemolytic anemia (abstract). Transfusion 1986;
tides carrying blood group antigens.
15. Des Roziers NB, Squalli S. Removing IgG antibodies
4. Issitt PD, Anstee DJ. Applied blood group serology.
from intact red cells: Comparison of acid and EDTA,
4th ed. Durham, NC: Montgomery Scientific
heat, and chloroquine elution methods. Transfusion
5. Judd WJ. Methods in immunohematology. 2nd ed.
16. Liew YW, Uchikawa M. Loss of Era antigen in very low
Durham, NC: Montgomery Scientific Publications,
pH buffers (letter). Transfusion 1987;27:442–3.
17. Champagne K, Spruell P, Chen J, et al. EDTA/glycine-
6. Alberts B, Bray D, Lewis J, et al. Molecular biology of
acid vs. chloroquine diphosphate treatment for strip-
the cell. 3rd ed. New York: Garland Publishing Co.,
ping Bg antigens from red blood cells (abstract).
7. Branch DR, Muensch HA, Sy Siok Hian AL, Petz LD.
18. Tanner MJA. The structure and function of band 3
Disulfide bonds are a requirement for Kell and
Cartwright (Yta ) blood group antigen integrity. Br J
19. Norris SS,Allen DD, Neff TP,Wilkinson SL. Evaluation
8. Branch DR, Petz LD. A new reagent (ZZAP) having
of 4,4'-diisothiocyanatostilbene-2,2'-disulfonic acid
multiple applications in immunohematology. Am J
in the inhibition of rouleaux formation. Transfusion
9. Mantel W, Holtz G. Characterisation of autoantibodies
20. Reid ME, Lomas-Francis C. The blood group antigen
to erythrocytes in autoimmune haemolytic anaemia
factsbook. San Diego:Academic Press, 1996.
by chloroquine. Vox Sang 1976;30:453–63.
21. Reid ME, Green CA, Hoffer J, Øyen R. Effect of
10. Swanson JL, Sastamoinen R. Chloroquine stripping of
pronase on high incidence blood group antigens and
the prevalence of antibodies to pronase-treated ery-
throcytes. Immunohematology 1996;12:139–42.
11. Giles CM, Darke C, Rowe GP, Botto M. HLA class I
(Bg) antigens on red cells of SLE patients: a serologi-
Jill R. Storry, PhD, FIBMS, Imunohematology
cal study with polyclonal and monoclonal antibod-
Laboratory, New York Blood Center, 310 East 67th
12. Sassetti R, Nichols D. Decreased antigenic reactivity
Vol. 16, No. 2, 2000 Improving transfusion safety by electronic identification of patients, blood samples, and blood units.
The authors have informed the editors of Imunohematology that there is an error on page 82, first paragraph,fourth sentence. The sentence should read “In the United States, the incidence of fatalities from transfusion ofwrong red cells or whole blood is estimated to be one per 600,000 transfusions.” We regret the error.
Significant ABO hemolytic diseaseof the newborn in a group B infantwith a group A mother
H. JEON, B. CALHOUN, M. POTHIAWALA, M. HERSCHEL,AND B.W. BARON
ABO hemolytic disease of the newborn (HDN) occurs almost exclusively in infants of blood group A or B who are born to group O mothersbecause IgG anti-A or -B occurs more commonly in group O than in group A or B individuals. We report a case in which clinically significantABO-HDN occurred in a group B neonate from anti-B of a group A mother. The IgG anti-B titer was much higher (256) than that found in a
group A mother/infant control group (≤ 32). The maternal antibody screen was negative and antibodies to low-frequency antigens were not
detected. Therefore, when evaluating unexplained HDN in a group B newborn of a group A mother, it may be relevant to determine the sub- group of the mother. As presented here, anti-B from a group A mother may, on occasion, be responsible for HDN. Immunohematology 2000;16: 105–108.
Moderate hemolytic disease of thenewborn due to anti-Hr in a mother
Hemolytic disease of the newborn (HDN) due to anti-Hr antibody is typically severe and often fatal. We report a case of moderate HDN due
to anti-Hr in a woman with the D––/D–– phenotype. A 33-year-old woman delivered her second child who was mildly jaundiced. The high-
est level of bilirubin was 26.1 mg/dL on the third day postpartum and the hemoglobin concentration was 14.0 g/dL. The newborn recoveredafter phototherapy and no mental retardation was noticed after 1 year of follow up. An exchange transfusion was excluded due to the lack ofa compatible donor and the physical condition of the mother precluded blood donation. The maternal RBCs were D+C–c–E–e–; only G andRh29 of the Rh system were expressed. Thus, her probable phenotype was D––/D––. Her alloantibody was identified as anti-Hr (anti-Rh17)
as it reacted with all red blood cells (RBCs) but not her own, other D--– RBCs, and Rh
RBCs. The results of the antibody titer (64) and activ-
ity in a chemiluminescense test (CLT; 34%) were consistent with a moderate HDN. Family studies were negative for the D––/D–– phenotypeand consanguinity was not proved. This is the first described case of moderate HDN due to anti-Hr . The result of antibody activity in the CLT
might be helpful in predicting the severity of HDN in other rare HDN cases. Immunohematology 2000;16:109–111.
A gel technology system todetermine postpartum RhIGdosage
J.R. FERNANDES, R. CHAN, A.S. COOVADIA, M.D. REIS, AND P.H. PINKERTON
Failures of Rh immune globulin (RhIG) prophylaxis occur when the dose is too small. We report a test using a gel technology (GT) method to replace the Kleihauer–Betke (K–B) test to assess fetomaternal hemorrhage (FMH) and assist in determining the minimum necessary dose of RhIG. Cord blood (O, D+) was mixed with adult blood (O D–) to mimic an FMH of 10 mL, 20 mL, 28 mL, and 40 mL. Test samples were incu- bated with anti-D at known concentrations and centrifuged. The supernatant was titrated against D+ and D– red cells using GT and an inter- pretation of the required RhIG dose was made. Results were compared with the K–B test. Results were easily discernible and interpretations leading to determination of recommended RhIG dosage were reproducible. Correlation to standard K–B testing was confirmed. Elapsed time for result availability by GT testing was 60 minutes, with a direct technical time requirement of 30 minutes. The GT system is easier, objec- tive, and quantitative, and compares well to the standard K–B test. A single procedure will allow assessment of the extent of FMH in the great majority of cases. This technique works well in determining the appropriate dose of anti-D required to treat D– patients with D+ newborns. There are potential cost savings in decreased use of RhIG, less direct technical time required, and more rapid availability of results. Immunohematology 2000;16:115–119.
A successful delivery of a babyfrom a D––/ D–– mother withstrong anti-Hr0
D.H.WHANG, H.C. KIM, M. HUR, J.H. CHOI, J.S. PARK,AND K.S. HAN
We describe the first reported case in Korea of a woman with a D––/ D–– phenotype, a high-titer anti-Hr , and the successful delivery of her
newborn. The mother had a history of spontaneous abortion and artificial termination. In her third pregnancy, a live infant was delivered, butdied of severe hemolytic disease of the newborn due to anti- Hr in spite of intensive medical intervention. In her fourth pregnancy, at 22 weeks
gestation, the titer of anti- Hr was 1024, fetal cells were direct antiglobulin test positive and the blood type was group O, D+ (CDe). We per-
formed plasma exchanges in the mother; however, the titer of antibody rebounded to its initial level after the third plasma exchange. At 26 weeks gestation, cord blood Hb decreased to 7.1 g/dL and three intrauterine transfusions were performed using the mother’s washed red blood cells (RBCs). At 34 weeks gestation, a live baby was delivered by cesarean section. The infant was hydropic with hyperbilirubinemia and severe anemia. However, after two exchange transfusions using the washed RBCs of the mother’s sister, who was also D––/D––, laboratory and clin- ical findings returned to normal. Immunohematology 2000;16:112–114.
Large-scale use of red blood cellunits containing alloantibodies
Many transfusion services are reluctant to accept red blood cell (RBC) units containing antibodies. We evaluated the impact of accepting rou- tine shipments of our region’s inventory of alloantibody-positive RBC units over a 4-month period. All patients’ samples received up to 30 days after transfusion of such units were evaluated for the presence of passively acquired antibody, and labor and reagent costs were determined. During the study period, we received 259 alloantibody-containing RBC units, and 253 of these were transfused to 187 patients. Follow-up sam- ples were received on 99 of these187 patients, and 10 of these patients had detectable passive antibody in posttransfusion antibody screening tests. Two patients had anti-C and -D and eight patients had anti-D. Due to our negotiation of a small discount for antibody-containing units and the use of 20 units based on labeled phenotype rather than antigen typing in our laboratory, we experienced a net savings of $3814 over the 4-month period. This savings was achieved despite some additional costs incurred, including costs of data entry and additional testing on patients’ samples. We concluded that large-scale use of RBC units from donors with alloantibodies is safe and likely to have a minimal impact on a busy transfusion service’s workload and costs. Furthermore, nationwide use of such units would help alleviate projected blood short- ages. Immunohematology 2000;16:120–123.
Stillen nach Brustoperationen Kölner Ringvortrag am 2.02.2010 1. Stillfähigkeit2. Mammareduktion3. Brustvergrößerung4. Verletzungen der Brust 5. Krebsoperationen und Bestrahlung6. Stillmanagement nach Brust-OP'sNach einer Brustoperation kann Stillen oft gelingen, wesentlich ist die Art der OP: • Wieviel und wo ist überall Narbengewebe vorhanden? • Wurden Milchgänge, Blutgefäße od
Ozone System is key to OPL’s savingsNursing Facility in New York using alternative sanitizer for laundry - producing higher quality finished linens and saving thousands of dollars a year and water costs by 65% and chemical costs Health Administration) inspected us, they couldnʼt believe it was a laundry. They the Hudson Valley has taken advantage of equipment manufactured by ClearWat
 A review: modification of the
A review: modification of the  Although proteases are more commonly used in
blood group serology, glycosidases (enzymes that cleavesugars) also may help determine an antigen’s character-istics.Table 1 lists the most commonly used enzymes andtheir substrates.
Although proteases are more commonly used in
blood group serology, glycosidases (enzymes that cleavesugars) also may help determine an antigen’s character-istics.Table 1 lists the most commonly used enzymes andtheir substrates.